

Relationship of Lung Function and Inspiratory Strength with Exercise Capacity and Prognosis in Heart Failure
- PMID: 35137780
- PMCID: PMC9006999
- DOI: 10.36660/abc.20201130
Relationship of Lung Function and Inspiratory Strength with Exercise Capacity and Prognosis in Heart Failure
Abstract
Background: Spirometry is underused in heart failure (HF) and the extent to which each defect associates with exercise capacity and prognosis is unclear.
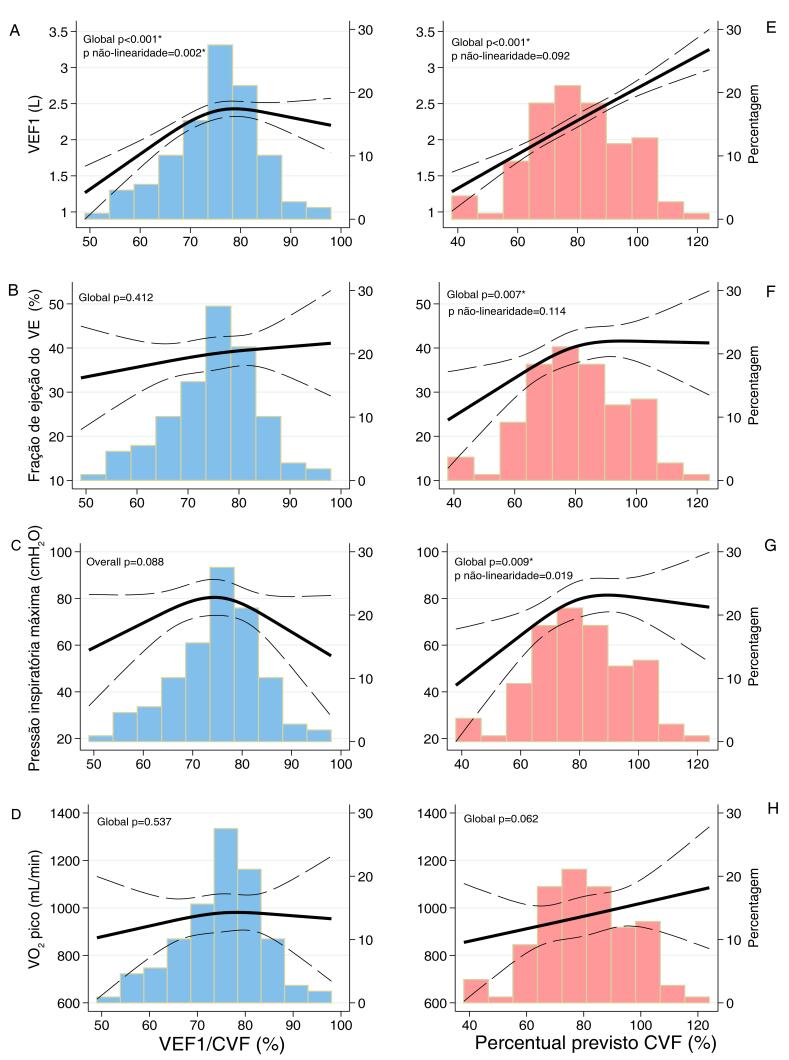
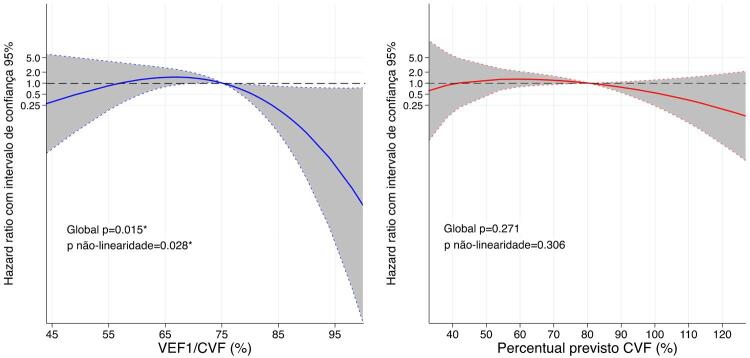
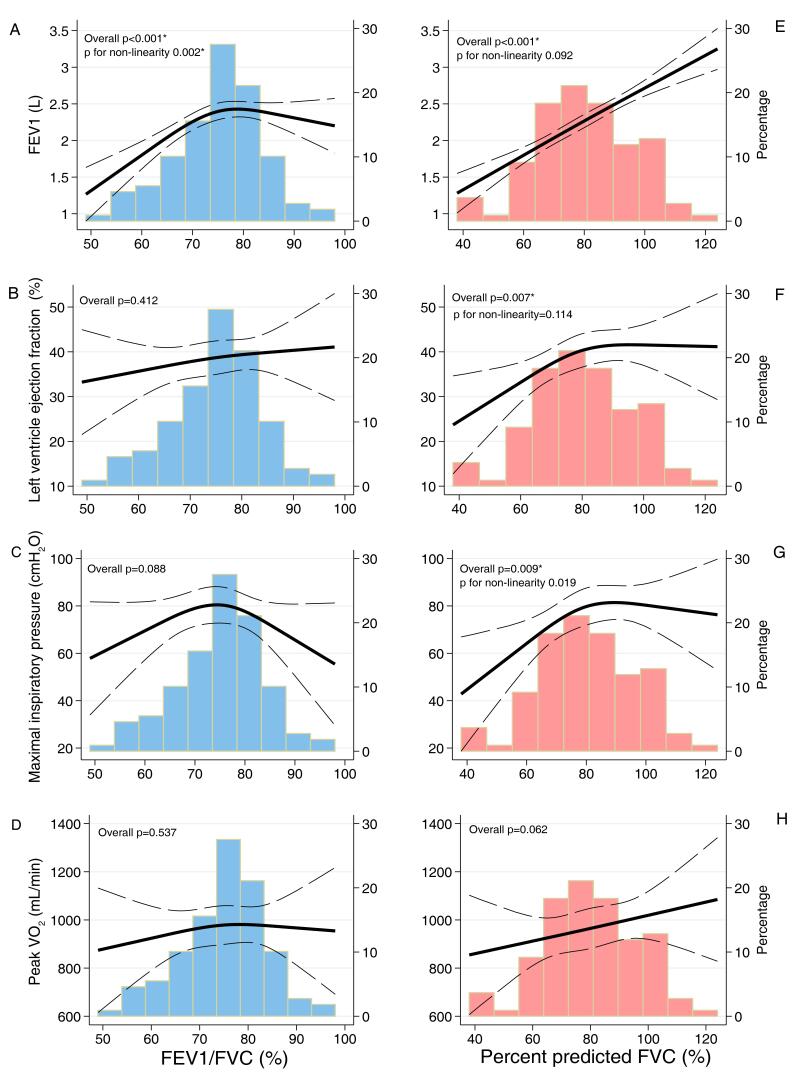
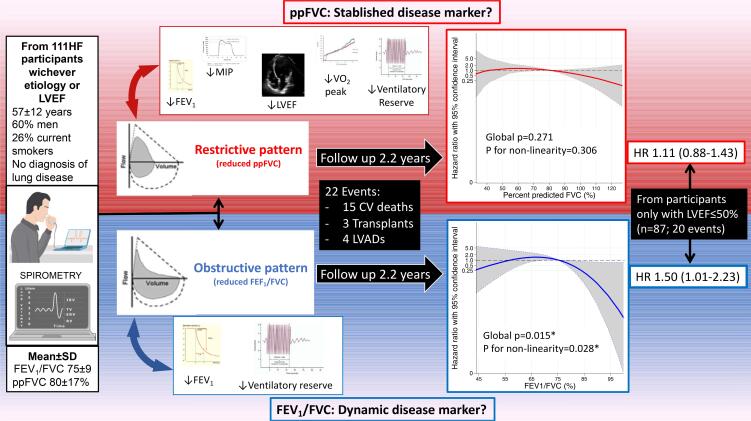
Objective: To determine the distinct relationship of continuous %predicted FVC (ppFVC) and FEV1/FVC with: 1) maximal inspiratory pressure (MIP), left ventricular ejection fraction (LVEF), exercise performance; and 2) prognosis for the composite of cardiovascular death, heart transplantation or left ventricular assist device implant.
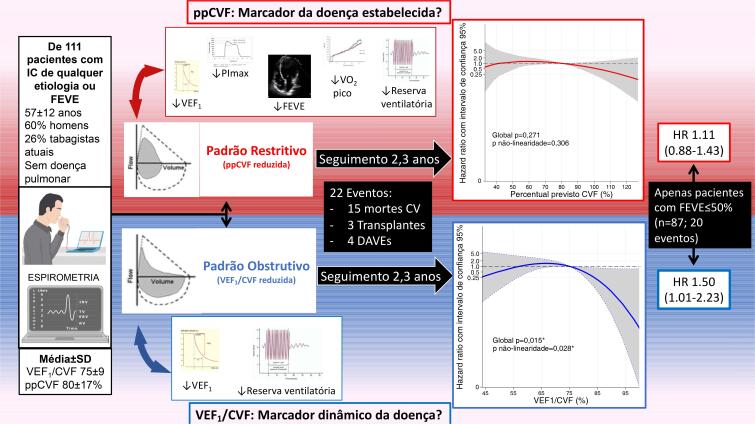
Methods: A cohort of 111 HF participants (AHA stages C/D) without diagnosed pneumopathy, spirometry, manovacuometry and maximum cardiopulmonary test. The association magnitudes were verified by linear and Cox (HR; 95% CI) regressions, age/sex adjusted. A p<0.05 was considered significant.
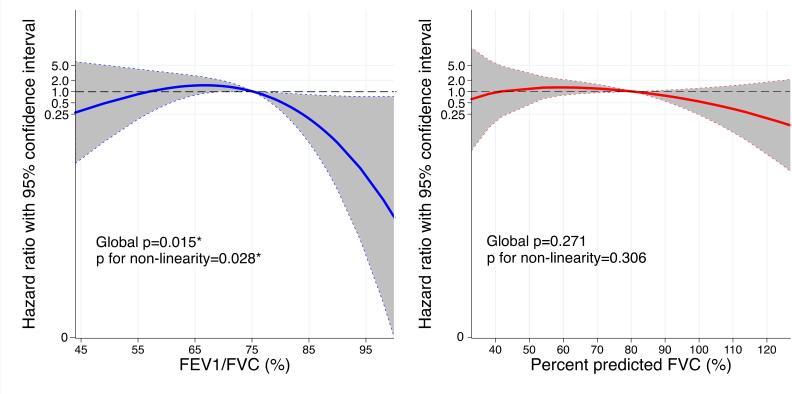
Results: Age was 57±12 years, 60% men, 64% in NYHA III. Every 10%-point increase in FEV1/FVC [β 7% (95% CI: 3-10)] and ppFVC [4% (2-6)] associated with ventilatory reserve (VRes), however only ppFVC associated with MIP [3.8 cmH2O (0.3-7.3)], LVEF [2.1% (0.5-3.8)] and VO2peak [0.5 mL/kg/min (0.1-1.0)], accounting for age/sex. In 2.2 years (mean), 22 events occurred, and neither FEV1/FVC (HR 1.44; 95% CI: 0.97-2.13) nor ppFVC (HR 1.13; 0.89-1.43) was significantly associated with the outcome. Only in the LVEF ≤50% subgroup (n=87, 20 events), FEV1/FVC (HR 1.50; 1.01-2.23), but not ppFVC, was associated with greater risk.
Conclusions: In chronic HF, reduced ppFVC associated with lower MIP, LVEF, VRes and VO2peak, but no distinct poorer prognosis over 2.2 years of follow-up. Distinctively, FEV1/FVC was associated only with VRes, and, in participants with LVEF ≤50%, FEV1/FVC reduction proportionally worsened prognosis. Therefore, FEV1/FVC and ppFVC add supplementary information regarding HF phenotyping.
Fundamento: A espirometria é subutilizada na insuficiência cardíaca (IC) e não está claro o grau de associação de cada defeito com a capacidade de exercício e com o prognóstico desses pacientes.
Objetivo: Determinar a relação da %CVF prevista (ppCVF) e do VEF1/CVF contínuos com: 1) pressão inspiratória máxima (PImáx), fração de ejeção do ventrículo esquerdo (FEVE) e desempenho ao exercício; e 2) prognóstico, para o desfecho composto de morte cardiovascular, transplante cardíaco ou implante de dispositivo de assistência ventricular.
Métodos: Coorte de 111 participantes com IC (estágios AHA C/D) sem pneumopatia; foram submetidos a espirometria, manovacuometria e teste cardiopulmonar máximo. As magnitudes de associação foram verificadas por regressões lineares e de Cox (HR; IC 95%), ajustadas para idade/sexo, e p <0,05 foi considerado significativo.
Resultados: Com idade média 57±12 anos, 60% eram homens, 64% em NYHAIII. A cada aumento de 10% no VEF1/CVF [β 7% (IC 95%: 3-10)] e no ppCVF [4% (2-6)], foi associado à reserva ventilatória (VRes); no entanto, apenas o ppCVF associado à PImáx [3,8cmH2O (0,3-7,3)], à fração de ejeção do ventrículo esquerdo (FEVE) [2,1% (0,5-3,8)] e ao VO2 pico [0,5mL/kg/min (0,1-1,0)], considerando idade/sexo. Em 2,2 anos (média), ocorreram 22 eventos; tanto FEV1/FVC (HR 1,44; IC 95%: 0,97-2,13) quanto ppCVF (HR 1,13; 0,89-1,43) não foram associados ao desfecho. Apenas no subgrupo FEVE ≤50% (n=87, 20 eventos), VEF1/CVF (HR 1,50; 1,01-2,23), mas não ppCVF, foi associado a risco.
Conclusão: Na IC crônica, ppCVF reduzido associou-se a menor PImáx, FEVE, VRes e VO2 pico, mas não distinguiu pior prognóstico em 2,2 anos de acompanhamento. Entretanto, VEF1/CVF associou-se apenas com VRes, e, em participantes com FEVE ≤50%, o VEF1/CVF reduzido mostrou pior prognóstico proporcional. Portanto, VEF1/CVF e ppFVC contribuem para melhor fenotipagem de pacientes com IC.
Conflict of interest statement
Potencial conflito de interesse
Não há conflito com o presente artigo
Figures
Comment in
-
Lung Function and Inspiratory Muscle Strength in Heart Failure: Can They be Considered Potential Prognostic Markers?Arq Bras Cardiol. 2022 Apr;118(4):692-693. doi: 10.36660/abc.20211060. Arq Bras Cardiol. 2022. PMID: 35508045 Free PMC article. English, Portuguese. No abstract available.
Similar articles
-
Association of Pulmonary Function With Late-Life Cardiac Function and Heart Failure Risk: The ARIC Study.J Am Heart Assoc. 2022 Jul 19;11(14):e023990. doi: 10.1161/JAHA.121.023990. Epub 2022 Jul 5. J Am Heart Assoc. 2022. PMID: 35861819 Free PMC article.
-
The prognostic significance of lung function in stable heart failure outpatients.Clin Cardiol. 2017 Nov;40(11):1145-1151. doi: 10.1002/clc.22802. Epub 2017 Sep 13. Clin Cardiol. 2017. PMID: 28902960 Free PMC article.
-
Preliminary investigation of cardiopulmonary function in stroke patients with stable heart failure and exertional dyspnea.Medicine (Baltimore). 2016 Oct;95(40):e5071. doi: 10.1097/MD.0000000000005071. Medicine (Baltimore). 2016. PMID: 27749577 Free PMC article.
-
Ivabradine Improves Cardiac Function and Increases Exercise Capacity in Patients with Chronic Heart Failure.Int Heart J. 2019 Jul 27;60(4):899-909. doi: 10.1536/ihj.18-559. Epub 2019 Jul 12. Int Heart J. 2019. PMID: 31308326
-
Impact of ivabradine on the cardiac function of chronic heart failure reduced ejection fraction: Meta-analysis of randomized controlled trials.Clin Cardiol. 2021 Apr;44(4):463-471. doi: 10.1002/clc.23581. Epub 2021 Feb 27. Clin Cardiol. 2021. PMID: 33638556 Free PMC article. Review.
Cited by
-
Effect of Enteral and Parenteral Nutrition Support on Pulmonary Function in Elderly Patients with Chronic Obstructive Pulmonary Disease Complicated by Respiratory Failure.Comput Math Methods Med. 2022 Oct 5;2022:4743070. doi: 10.1155/2022/4743070. eCollection 2022. Comput Math Methods Med. 2022. Retraction in: Comput Math Methods Med. 2023 Dec 6;2023:9878450. doi: 10.1155/2023/9878450. PMID: 36245845 Free PMC article. Retracted.
-
Lung Function and Inspiratory Muscle Strength in Heart Failure: Can They be Considered Potential Prognostic Markers?Arq Bras Cardiol. 2022 Apr;118(4):692-693. doi: 10.36660/abc.20211060. Arq Bras Cardiol. 2022. PMID: 35508045 Free PMC article. English, Portuguese. No abstract available.
References
-
- Neder JA, Rocha A, Berton DC, O’Donnell DE. Clinical and Physiologic Implications of Negative Cardiopulmonary Interactions in Coexisting Chronic Obstructive Pulmonary Disease-Heart Failure. Clin Chest Med. 2019;40(2):421-38. doi: 10.1016/j.ccm.2019.02.006. - PubMed
- Neder JA, Rocha A, Berton DC, O’Donnell DE. Clinical and Physiologic Implications of Negative Cardiopulmonary Interactions in Coexisting Chronic Obstructive Pulmonary Disease-Heart Failure. 10.1016/j.ccm.2019.02.006.Clin Chest Med. 2019;40(2):421–438. - PubMed
-
- Cundrle I Jr, Olson LJ, Johnson BD. Pulmonary Limitations in Heart Failure. Clin Chest Med. 2019;40(2):439-48. doi: 10.1016/j.ccm.2019.02.010. - PMC - PubMed
- Cundrle I, Jr, Olson LJ, Johnson BD. Pulmonary Limitations in Heart Failure. 10.1016/j.ccm.2019.02.010.Clin Chest Med. 2019;40(2):439–448. - PMC - PubMed
-
- Lalande S, Cross TJ, Keller-Ross ML, Morris NR, Johnson BD, Taylor BJ. Exercise Intolerance in Heart Failure: Central Role for the Pulmonary System. Exerc Sport Sci Rev. 2020;48(1):11-9. doi: 10.1249/JES.0000000000000208. - PMC - PubMed
- Lalande S, Cross TJ, Keller-Ross ML, Morris NR, Johnson BD, Taylor BJ. Exercise Intolerance in Heart Failure: Central Role for the Pulmonary System. 10.1249/JES.0000000000000208.Exerc Sport Sci Rev. 2020;48(1):11–19. - PMC - PubMed
-
- Canepa M, Straburzynska-Migaj E, Drozdz J, Fernandez-Vivancos C, Pinilla JMG, Nyolczas N, et al. Characteristics, Treatments and 1-year Prognosis of Hospitalized and Ambulatory Heart Failure Patients with Chronic Obstructive Pulmonary Disease in the European Society of Cardiology Heart Failure Long-Term Registry. Eur J Heart Fail. 2018;20(1):100-10. doi: 10.1002/ejhf.964. - PubMed
- Canepa M, Straburzynska-Migaj E, Drozdz J, Fernandez-Vivancos C, Pinilla JMG, Nyolczas N, et al. Characteristics, Treatments and 1-year Prognosis of Hospitalized and Ambulatory Heart Failure Patients with Chronic Obstructive Pulmonary Disease in the European Society of Cardiology Heart Failure Long-Term Registry. 10.1002/ejhf.964.Eur J Heart Fail. 2018;20(1):100–110. - PubMed
-
- Lawson CA, Mamas MA, Jones PW, Teece L, McCann G, Khunti K, et al. Association of Medication Intensity and Stages of Airflow Limitation With the Risk of Hospitalization or Death in Patients with Heart Failure and Chronic Obstructive Pulmonary Disease. JAMA Netw Open. 2018;1(8):e185489. doi: 10.1001/jamanetworkopen.2018.5489. - PMC - PubMed
- Lawson CA, Mamas MA, Jones PW, Teece L, McCann G, Khunti K, et al. Association of Medication Intensity and Stages of Airflow Limitation With the Risk of Hospitalization or Death in Patients with Heart Failure and Chronic Obstructive Pulmonary Disease. 10.1001/jamanetworkopen.2018.5489.JAMA Netw Open. 2018;1(8):e185489. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
