

Effectiveness of Unguided Internet-Based Cognitive Behavioral Therapy and the Three Good Things Exercise for Insomnia: 3-Arm Randomized Controlled Trial
- PMID: 35138259
- PMCID: PMC8867295
- DOI: 10.2196/28747
Effectiveness of Unguided Internet-Based Cognitive Behavioral Therapy and the Three Good Things Exercise for Insomnia: 3-Arm Randomized Controlled Trial
Abstract
Background: The treatment of insomnia with sleep medication causes problems such as long-term use, dependence, and significant economic losses, including medical expenses. Evidence-based lifestyle guidance is required to improve insomnia symptoms not only in person but also in easy-to-use web-based formats.
Objective: This study aims to clarify whether unguided internet-based cognitive behavioral therapy (ICBT) or the Three Good Things (TGT) exercise, both administered as self-help internet interventions without email support, could improve insomnia symptoms compared with a waiting list control (WLC) group.
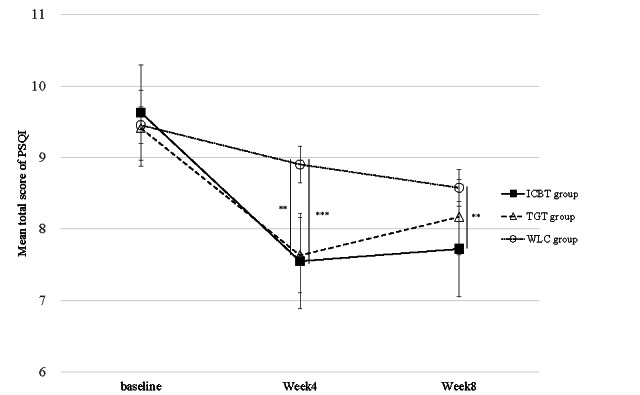
Methods: A 4-week program was implemented, and participants were randomly allocated to 1 of the 3 groups. The primary outcome measure was the Pittsburgh Sleep Questionnaire (PSQI) score at 4 weeks compared with baseline.
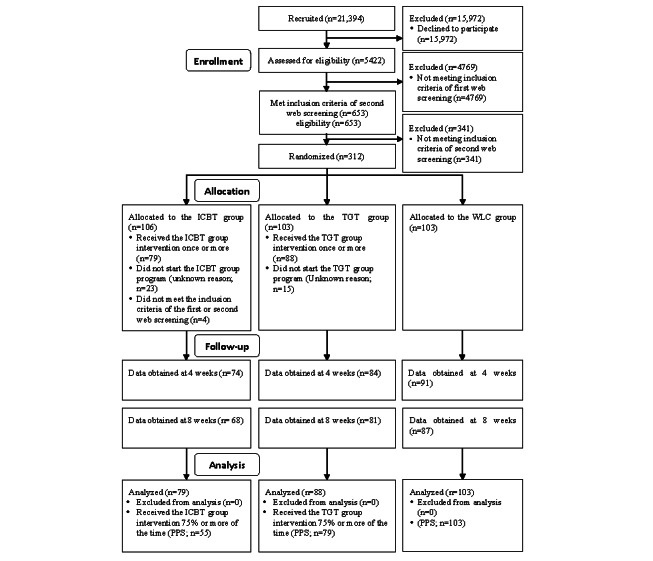
Results: Of the 21,394 individuals invited to participate, 312 (1.46%) met the eligibility criteria and were randomly assigned to 1 of the 3 groups. Of these 312 individuals, 270 (86.5%; ICBT 79/270, 29.3%; TGT 88/270, 32.6%; and WLC 103/270, 38.1%) completed a postintervention survey at 4 and 8 weeks. The adjusted mean changes of the primary outcome measure (PSQI) in the ICBT (-1.56, 95% CI -2.52 to -0.59; P<.001) and TGT (-1.15, 95% CI -2.08 to -0.23; P=.002) groups at 4 weeks from baseline showed a significant improvement compared with the WLC group. The adjusted mean changes in the secondary outcome measures of sleep onset latency, total sleep time, Athens Insomnia Scale score, and Patient Health Questionnaire-9 score at 4 weeks from baseline, as well as in the PSQI at 8 weeks from baseline, showed significant improvement for ICBT. Moreover, total sleep time, Athens Insomnia Scale, and Patient Health Questionnaire-9 scores at 4 weeks from baseline showed a significant improvement in the TGT group compared with the WLC group.
Conclusions: A total of 4 weeks of unguided ICBT and TGT exercises improved insomnia.
Trial registration: University Hospital Medical Information Network Clinical Trial Registry UMIN000034927; https://center6.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000039814.
Keywords: cognitive behavioral therapy; insomnia; internet-based treatment; mobile phone; positive psychology; randomized controlled trial.
©Daisuke Sato, Yoichi Sekizawa, Chihiro Sutoh, Yoshiyuki Hirano, Sho Okawa, Motohisa Hirose, Ryo Takemura, Eiji Shimizu. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 09.02.2022.
Conflict of interest statement
Conflicts of Interest: SD and ES have developed the web-based treatment but have no commercial interests.
Figures
Similar articles
-
Effectiveness of Internet-Delivered Computerized Cognitive Behavioral Therapy for Patients With Insomnia Who Remain Symptomatic Following Pharmacotherapy: Randomized Controlled Exploratory Trial.J Med Internet Res. 2019 Apr 11;21(4):e12686. doi: 10.2196/12686. J Med Internet Res. 2019. PMID: 30973344 Free PMC article. Clinical Trial.
-
Efficacy of a Self-Guided Internet Intervention With Optional On-Demand Feedback Versus Digital Psychoeducation on Sleep Hygiene for University Students With Insomnia: Randomized Controlled Trial.J Med Internet Res. 2025 May 8;27:e58024. doi: 10.2196/58024. J Med Internet Res. 2025. PMID: 40341194 Free PMC article. Clinical Trial.
-
Effectiveness of Cognitive Behavioral Therapy Provided Through a Web Application for Subthreshold Depression, Subthreshold Insomnia, and Subthreshold Panic: Open-Labeled 6-Arm Randomized Clinical Trial Pilot Study.JMIR Form Res. 2025 Feb 3;9:e63139. doi: 10.2196/63139. JMIR Form Res. 2025. PMID: 39899369 Free PMC article. Clinical Trial.
-
Efficacy of online and face-to-face cognitive behavioral therapy in the treatment of neurological insomnia: a systematic review and meta-analysis.Ann Palliat Med. 2021 Oct;10(10):10684-10696. doi: 10.21037/apm-21-2387. Ann Palliat Med. 2021. PMID: 34763429
-
Does exercise improve sleep for adults with insomnia? A systematic review with quality appraisal.Clin Psychol Rev. 2019 Mar;68:1-12. doi: 10.1016/j.cpr.2018.11.002. Epub 2018 Nov 16. Clin Psychol Rev. 2019. PMID: 30617012
Cited by
-
Financial toxicity-related factors in patients with nasopharyngeal carfcinoma: a cross-sectional study.Support Care Cancer. 2025 Feb 19;33(3):201. doi: 10.1007/s00520-025-09273-4. Support Care Cancer. 2025. PMID: 39969642
-
Systematic review and meta-analysis on fully automated digital cognitive behavioral therapy for insomnia.NPJ Digit Med. 2025 Mar 12;8(1):157. doi: 10.1038/s41746-025-01514-4. NPJ Digit Med. 2025. PMID: 40075149 Free PMC article.
-
Treatment strategies for insomnia in Japanese primary care physicians' practice: A Web-based questionnaire survey.BMC Prim Care. 2024 Jun 18;25(1):219. doi: 10.1186/s12875-024-02449-7. BMC Prim Care. 2024. PMID: 38890610 Free PMC article.
-
Influencing factors of length of stay among repeatedly hospitalized patients with mood disorders: a longitudinal study in China.Ann Gen Psychiatry. 2024 Apr 25;23(1):15. doi: 10.1186/s12991-024-00497-y. Ann Gen Psychiatry. 2024. PMID: 38664741 Free PMC article.
-
"Three Good Things" Digital Intervention Among Health Care Workers: A Randomized Controlled Trial.Ann Fam Med. 2023 May-Jun;21(3):220-226. doi: 10.1370/afm.2963. Ann Fam Med. 2023. PMID: 37217328 Free PMC article. Clinical Trial.
References
-
- Diagnostic and Statistical Manual of Mental Disorders (DSM-5®) Washington, D.C: American Psychiatric Association; 2013. - PubMed
-
- Komada Y, Nomura T, Kusumi M, Nakashima K, Okajima I, Sasai T, Inoue Y. Correlations among insomnia symptoms, sleep medication use and depressive symptoms. Psychiatry Clin Neurosci. 2011 Feb;65(1):20–9. doi: 10.1111/j.1440-1819.2010.02154.x. doi: 10.1111/j.1440-1819.2010.02154.x. - DOI - DOI - PubMed
-
- Kim K, Uchiyama M, Okawa M, Liu X, Ogihara R. An epidemiological study of insomnia among the Japanese general population. Sleep. 2000 Feb 01;23(1):41–7. - PubMed
-
- Hafner M, Stepanek M, Taylor J, Troxel WM, van Stolk C. Why sleep matters-the economic costs of insufficient sleep: a cross-country comparative analysis. Rand Health Q. 2017 Jan;6(4):11. http://europepmc.org/abstract/MED/28983434 - PMC - PubMed
Publication types
MeSH terms
Associated data
- Actions
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
