

Quantitative classification and radiomics of [18F]FDG-PET/CT in indeterminate thyroid nodules
- PMID: 35138444
- PMCID: PMC9165273
- DOI: 10.1007/s00259-022-05712-0
Quantitative classification and radiomics of [18F]FDG-PET/CT in indeterminate thyroid nodules
Abstract
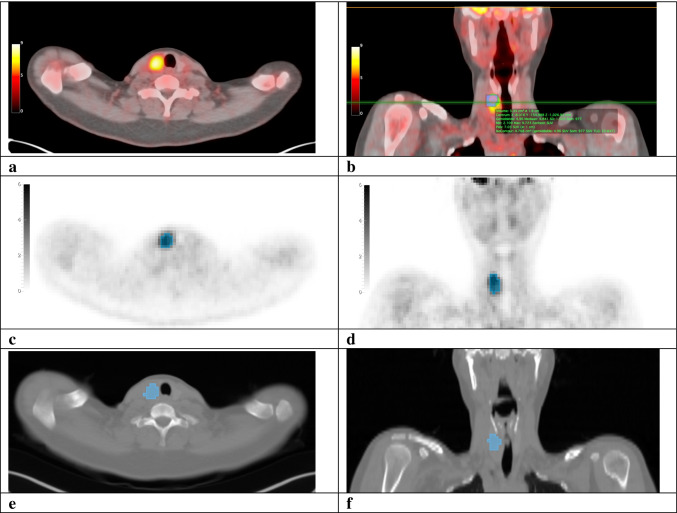
Purpose: To evaluate whether quantitative [18F]FDG-PET/CT assessment, including radiomic analysis of [18F]FDG-positive thyroid nodules, improved the preoperative differentiation of indeterminate thyroid nodules of non-Hürthle cell and Hürthle cell cytology.
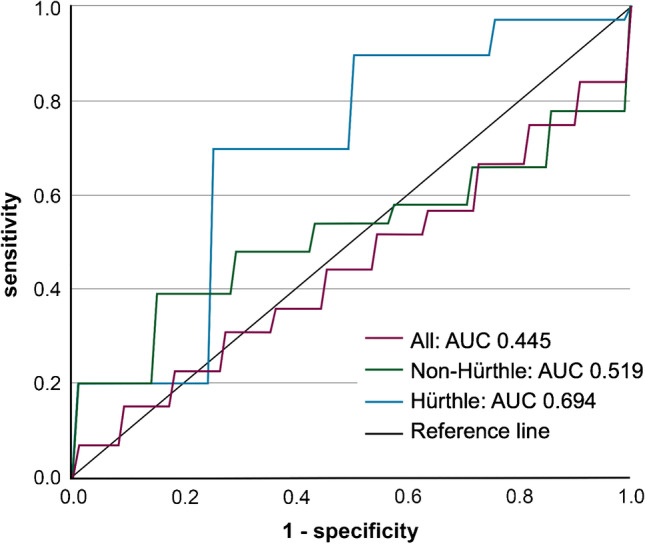
Methods: Prospectively included patients with a Bethesda III or IV thyroid nodule underwent [18F]FDG-PET/CT imaging. Receiver operating characteristic (ROC) curve analysis was performed for standardised uptake values (SUV) and SUV-ratios, including assessment of SUV cut-offs at which a malignant/borderline neoplasm was reliably ruled out (≥ 95% sensitivity). [18F]FDG-positive scans were included in radiomic analysis. After segmentation at 50% of SUVpeak, 107 radiomic features were extracted from [18F]FDG-PET and low-dose CT images. Elastic net regression classifiers were trained in a 20-times repeated random split. Dimensionality reduction was incorporated into the splits. Predictive performance of radiomics was presented as mean area under the ROC curve (AUC) across the test sets.
Results: Of 123 included patients, 84 (68%) index nodules were visually [18F]FDG-positive. The malignant/borderline rate was 27% (33/123). SUV-metrices showed AUCs ranging from 0.705 (95% CI, 0.601-0.810) to 0.729 (0.633-0.824), 0.708 (0.580-0.835) to 0.757 (0.650-0.864), and 0.533 (0.320-0.747) to 0.700 (0.502-0.898) in all (n = 123), non-Hürthle (n = 94), and Hürthle cell (n = 29) nodules, respectively. At SUVmax, SUVpeak, SUVmax-ratio, and SUVpeak-ratio cut-offs of 2.1 g/mL, 1.6 g/mL, 1.2, and 0.9, respectively, sensitivity of [18F]FDG-PET/CT was 95.8% (95% CI, 78.9-99.9%) in non-Hürthle cell nodules. In Hürthle cell nodules, cut-offs of 5.2 g/mL, 4.7 g/mL, 3.4, and 2.8, respectively, resulted in 100% sensitivity (95% CI, 66.4-100%). Radiomic analysis of 84 (68%) [18F]FDG-positive nodules showed a mean test set AUC of 0.445 (95% CI, 0.290-0.600) for the PET model.
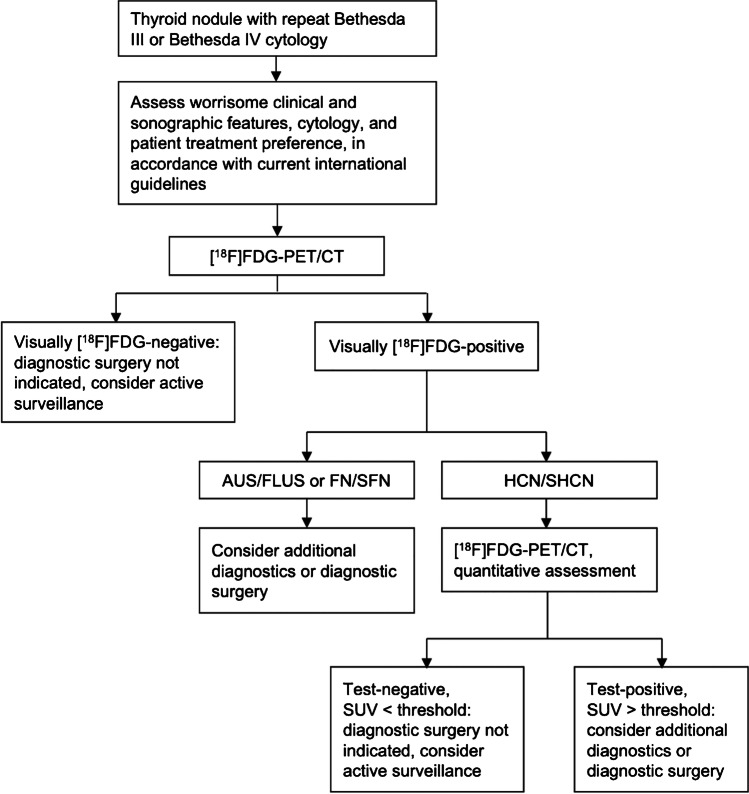
Conclusion: Quantitative [18F]FDG-PET/CT assessment ruled out malignancy in indeterminate thyroid nodules. Distinctive, higher SUV cut-offs should be applied in Hürthle cell nodules to optimize rule-out ability. Radiomic analysis did not contribute to the additional differentiation of [18F]FDG-positive nodules.
Trial registration number: This trial is registered with ClinicalTrials.gov: NCT02208544 (5 August 2014), https://clinicaltrials.gov/ct2/show/NCT02208544 .
Keywords: Indeterminate; Quantitative; Radiomics; Standardised uptake value; Thyroid carcinoma; Thyroid cytology; Thyroid nodule; [18F]FDG-PET/CT.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- de Koster EJ, de Geus-Oei LF, Brouwers AH, van Dam EWCM, Dijkhorst-Oei LT, van Engen-van Grunsven ACH, et al. [18F]FDG-PET/CT to prevent futile surgery in indeterminate thyroid nodules: a blinded, randomised controlled multicentre trial. Eur J Nucl Med Mol Imaging 2022. 10.1007/s00259-021-05627-2. - PMC - PubMed
-
- de Geus-Oei LF, Pieters GF, Bonenkamp JJ, Mudde AH, Bleeker-Rovers CP, Corstens FH, et al. 18F-FDG PET reduces unnecessary hemithyroidectomies for thyroid nodules with inconclusive cytologic results. J Nucl Med. 2006;47:770–775. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
