

Heart failure with preserved ejection fraction in patients with normal natriuretic peptide levels is associated with increased morbidity and mortality
- PMID: 35139159
- PMCID: PMC9649913
- DOI: 10.1093/eurheartj/ehab911
Heart failure with preserved ejection fraction in patients with normal natriuretic peptide levels is associated with increased morbidity and mortality
Abstract
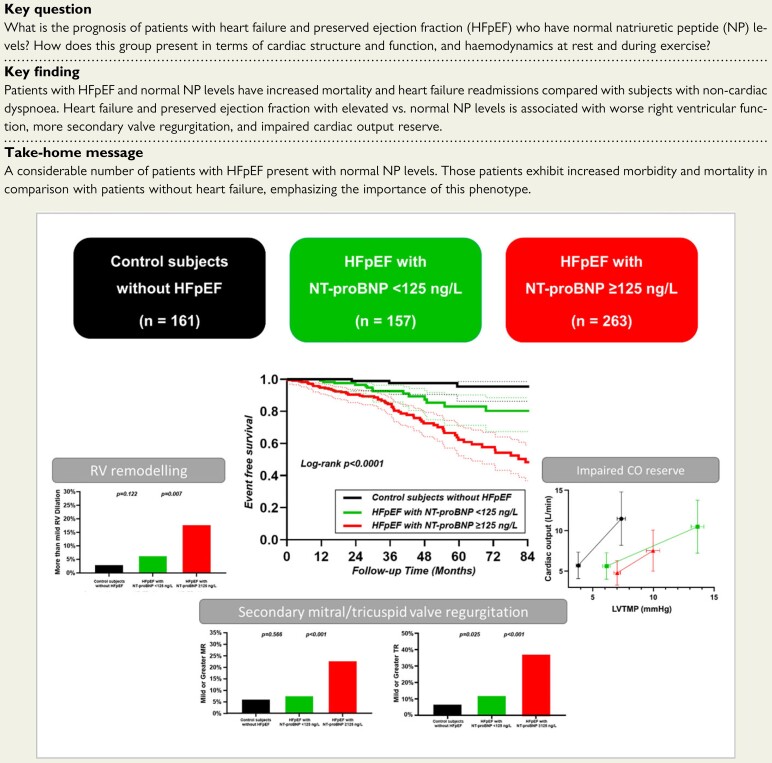
Background: A substantial proportion of patients with heart failure (HF) with preserved ejection fraction (HFpEF) present with normal natriuretic peptide (NP) levels. The pathophysiology and natural history for this phenotype remain unclear.
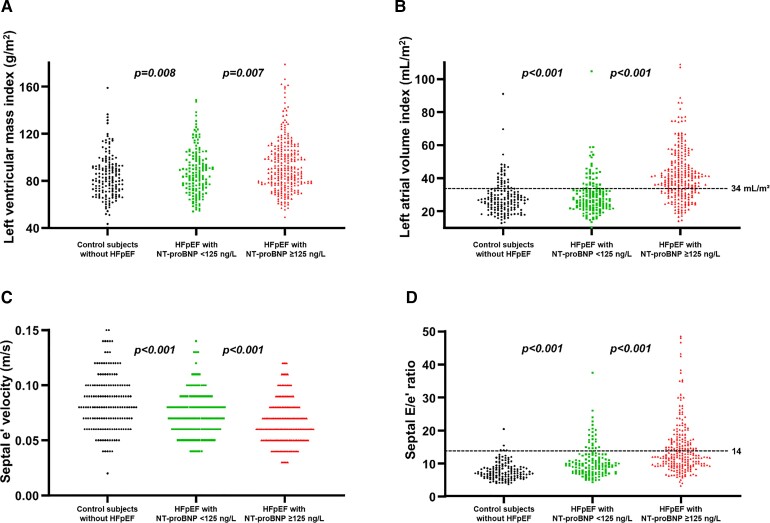
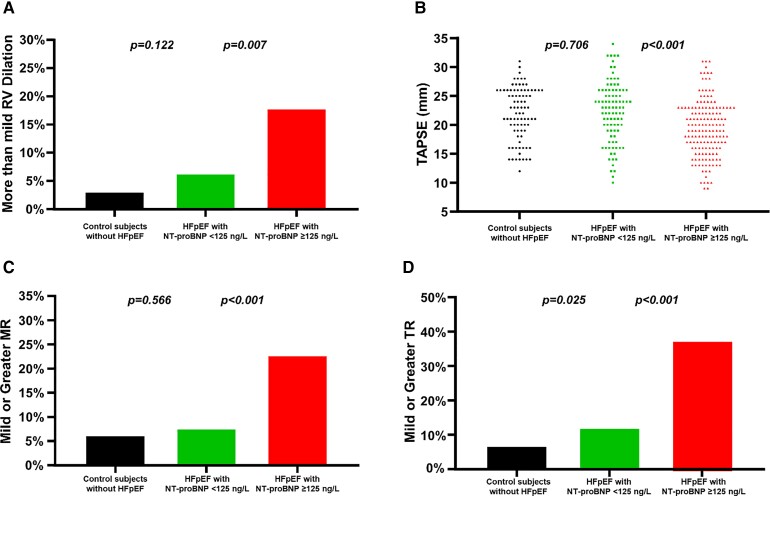
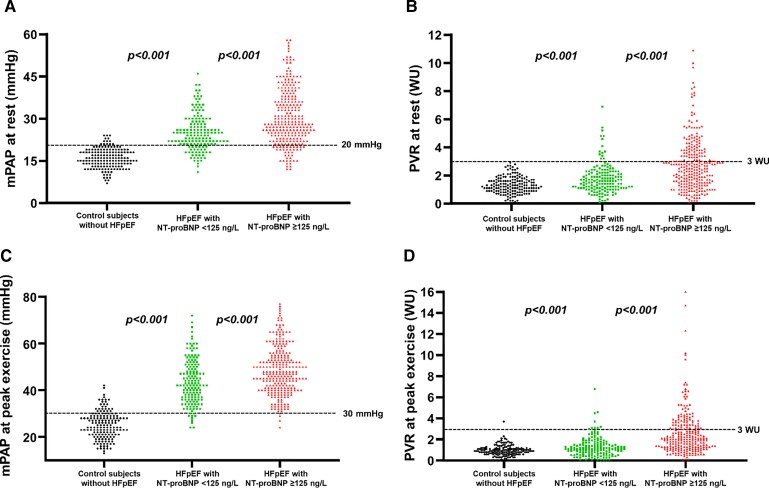
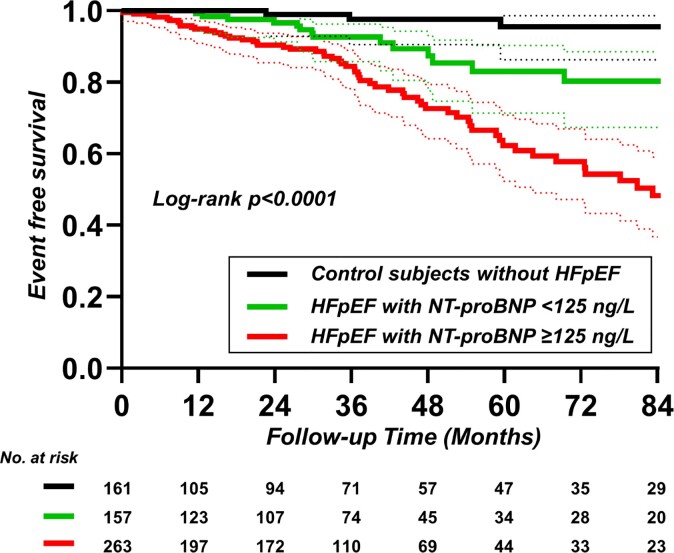
Methods and results: Consecutive subjects undergoing invasive cardiopulmonary exercise testing for unexplained dyspnoea at Mayo Clinic in 2006-18 were studied. Heart failure with preserved ejection fraction was defined as a pulmonary arterial wedge pressure (PAWP) ≥15 mmHg (rest) or ≥25 mmHg (exercise). Patients with HFpEF and normal NP [N-terminal of the pro-hormone B-type natriuretic peptide (NT-proBNP) < 125 ng/L] were compared with HFpEF with high NP (NT-proBNP ≥ 125 ng/L) and controls with normal haemodynamics. Patients with HFpEF and normal (n = 157) vs. high NP (n = 263) were younger, yet older than controls (n = 161), with an intermediate comorbidity profile. Normal NP HFpEF was associated with more left ventricular hypertrophy and worse diastolic function compared with controls, but better diastolic function, lower left atrial volumes, superior right ventricular function, and less mitral/tricuspid regurgitation compared with high NP HFpEF. Cardiac output (CO) reserve with exercise was preserved in normal NP HFpEF [101% predicted, interquartile range (IQR): 75-124%], but this was achieved only at the cost of higher left ventricular transmural pressure (LVTMP) (14 ± 6 mmHg vs. 7 ± 4 mmHg in controls, P < 0.001). In contrast, CO reserve was decreased in high NP HFpEF (85% predicted, IQR: 59-109%), with lower LVTMP (10 ± 8 mmHg) compared with normal NP HFpEF (P < 0.001), despite similar PAWP. Patients with high NP HFpEF displayed the highest event rates, but normal NP HFpEF still had 2.7-fold higher risk for mortality or HF readmissions compared with controls (hazard ratio: 2.74, 95% confidence interval: 1.02-7.32) after adjusting for age, sex, and body mass index.
Conclusion: Patients with HFpEF and normal NP display mild diastolic dysfunction and preserved CO reserve during exercise, despite marked elevation in filling pressures. While clinical outcomes are not as poor compared with patients with high NP, patients with normal NP HFpEF exhibit increased risk of death or HF readmissions compared with patients without HF, emphasizing the importance of this phenotype.
Keywords: Diastolic heart failure; Exercise tolerance; Mortality; Natriuretic peptides; Obesity.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
BNP: Biomarker Not Perfect in heart failure with preserved ejection fraction.Eur Heart J. 2022 May 21;43(20):1952-1954. doi: 10.1093/eurheartj/ehac121. Eur Heart J. 2022. PMID: 35301541 No abstract available.
-
So-far overlooked HFpEF patients with normal natriuretic peptide level need more evidence.ESC Heart Fail. 2022 Oct;9(5):3659-3660. doi: 10.1002/ehf2.14047. Epub 2022 Jun 21. ESC Heart Fail. 2022. PMID: 35729714 Free PMC article. No abstract available.
References
-
- Pieske B, Tschope C, de Boer RA, Fraser AG, Anker SD, Donal E, et al. How to diagnose heart failure with preserved ejection fraction: the HFA–PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur Heart J 2019;40:3297–3317. - PubMed
-
- Bozkurt B, Coats AJS, Tsutsui H, Abdelhamid CM, Adamopoulos S, Albert N, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and writing committee of the universal definition of heart failure: endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail 2021;23:352–380. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
