

A recurrent machine learning model predicts intracranial hypertension in neurointensive care patients
- PMID: 35139181
- PMCID: PMC9486888
- DOI: 10.1093/brain/awab453
A recurrent machine learning model predicts intracranial hypertension in neurointensive care patients
Abstract
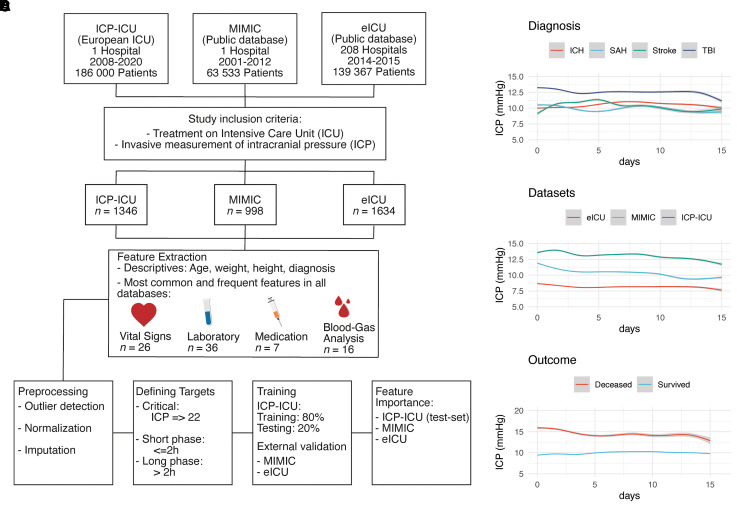
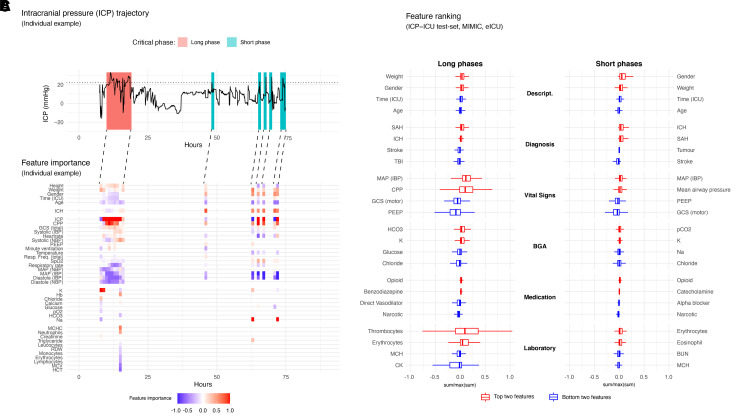
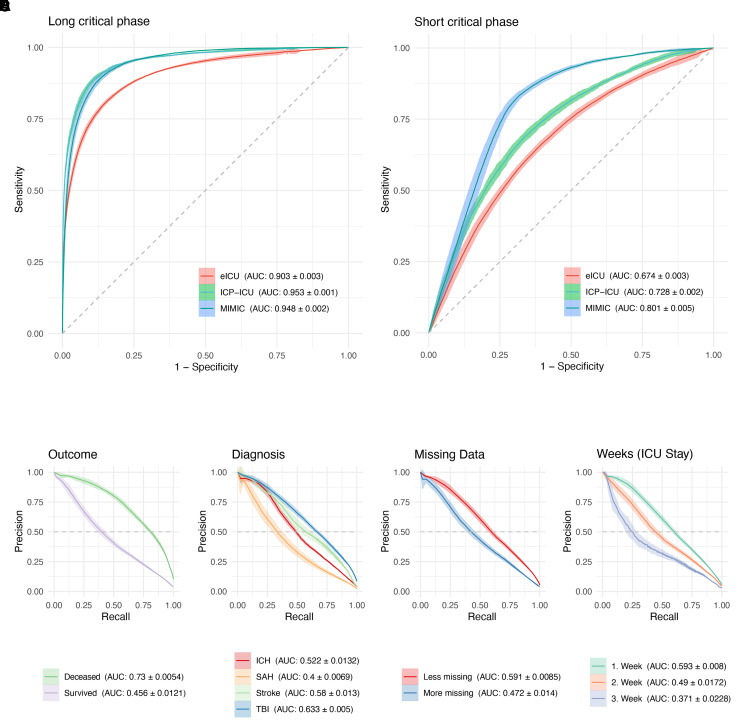
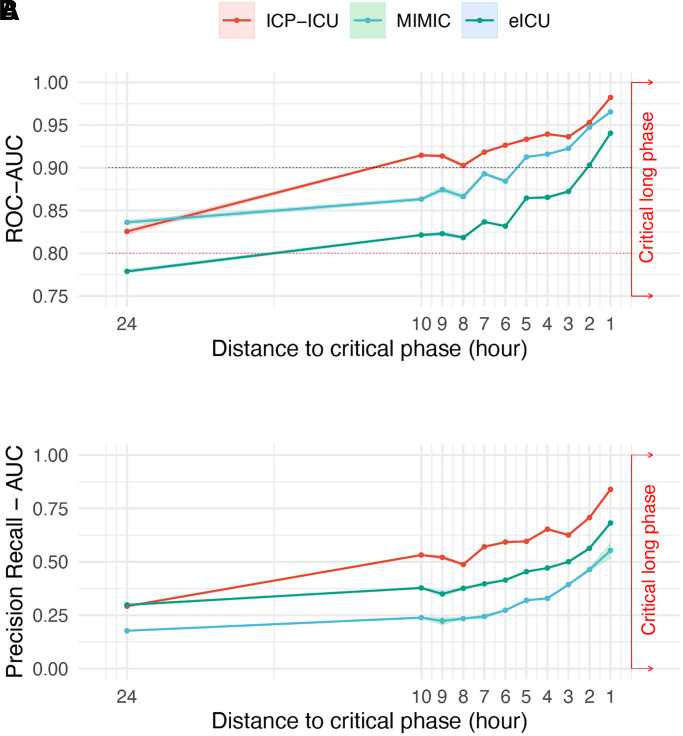
The evolution of intracranial pressure (ICP) of critically ill patients admitted to a neurointensive care unit (ICU) is difficult to predict. Besides the underlying disease and compromised intracranial space, ICP is affected by a multitude of factors, many of which are monitored on the ICU, but the complexity of the resulting patterns limits their clinical use. This paves the way for new machine learning techniques to assist clinical management of patients undergoing invasive ICP monitoring independent of the underlying disease. An institutional cohort (ICP-ICU) of patients with invasive ICP monitoring (n = 1346) was used to train recurrent machine learning models to predict the occurrence of ICP increases of ≥22 mmHg over a long (>2 h) time period in the upcoming hours. External validation was performed on patients undergoing invasive ICP measurement in two publicly available datasets [Medical Information Mart for Intensive Care (MIMIC, n = 998) and eICU Collaborative Research Database (n = 1634)]. Different distances (1-24 h) between prediction time point and upcoming critical phase were evaluated, demonstrating a decrease in performance but still robust AUC-ROC with larger distances (24 h AUC-ROC: ICP-ICU 0.826 ± 0.0071, MIMIC 0.836 ± 0.0063, eICU 0.779 ± 0.0046, 1 h AUC-ROC: ICP-ICU 0.982 ± 0.0008, MIMIC 0.965 ± 0.0010, eICU 0.941 ± 0.0025). The model operates on sparse hourly data and is stable in handling variable input lengths and missingness through its nature of recurrence and internal memory. Calculation of gradient-based feature importance revealed individual underlying decisions for our long short time memory-based model and thereby provided improved clinical interpretability. Recurrent machine learning models have the potential to be an effective tool for the prediction of ICP increases with high translational potential.
Keywords: deep learning; intensive care unit; intracranial pressure; machine learning; traumatic brain injury.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56. - PubMed
-
- Komorowski M, Celi LA, Badawi O, Gordon AC, Faisal AA. The Artificial Intelligence Clinician learns optimal treatment strategies for sepsis in intensive care. Nat Med. 2018;24(11):1716–1720. - PubMed
