

FGF23-Klotho Axis and Fractures in Patients Without and With Early CKD: A Case-Cohort Analysis of CARTaGENE
- PMID: 35139204
- PMCID: PMC9113817
- DOI: 10.1210/clinem/dgac071
FGF23-Klotho Axis and Fractures in Patients Without and With Early CKD: A Case-Cohort Analysis of CARTaGENE
Abstract
Context: Whether fibroblast growth factor-23 (FGF23) and α-Klotho are associated with fractures, especially in chronic kidney disease (CKD), remains controversial.
Objective: We evaluated how FGF23, α-Klotho, and traditional mineral parameters predict fractures in individuals with and without early CKD.
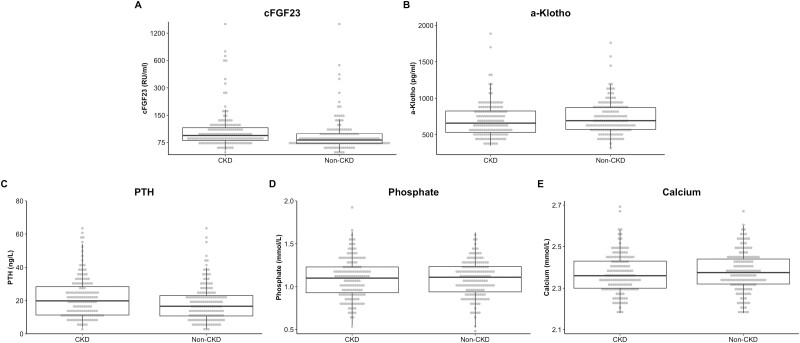
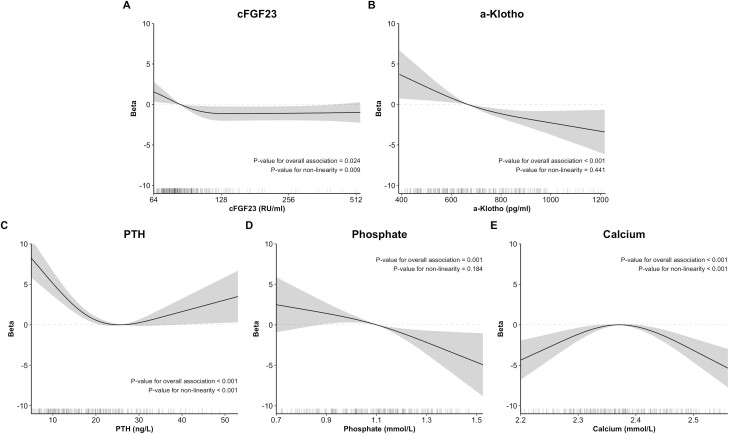
Methods: We conducted a stratified case-cohort analysis using CARTaGENE, a population-based survey from Quebec, Canada. Individuals aged 40 to 69 years were selected according to outcome and CKD status (non-CKD: eGFR > 60 mL/min/1.73 m2; CKD stage 3: eGFR 30-60 mL/min/1.73 m2]). Baseline levels of c-terminal FGF23 (cFGF23), α-Klotho, parathyroid hormone (PTH), phosphate, and calcium were analyzed for associations with osteoporotic fracture incidence from recruitment (2009-2010) through March 2016. Adjusted Cox models were used, and predictors were treated linearly or flexibly using splines.
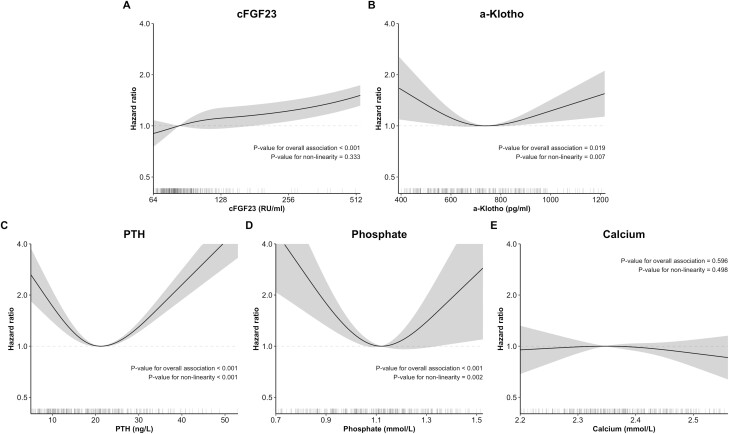
Results: A total of 312 patients (159 non-CKD; 153 CKD) were included; 98 had ≥ 1 fracture at any site during a median follow up of 70 months. Compared with non-CKD, CKD patients had increased levels of cFGF23 but similar levels of α-Klotho. cFGF23 was linearly associated with increased fracture incidence (adjusted HR = 1.81 [1.71, 1.93] per doubling for all participants). The association of α-Klotho with fracture followed a U-curve (overall P = 0.019) but was attenuated by adjustment for potential mediators (bone mineral density, phosphate, PTH). PTH and phosphate also had U-shaped associations with fracture. Associations were mostly similar between non-CKD and CKD. Adjustment for cFGF23 strongly attenuated the association between CKD status and fractures.
Conclusion: cFGF23 is associated linearly with fracture incidence while α-Klotho, PTH, and phosphate levels have a U-shaped association.
Keywords: FGF23; chronic kidney disease; fracture; parathyroid hormone; α-Klotho.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures

References
-
- Brenneman SK, Barrett-Connor E, Sajjan S, Markson LE, Siris ES. Impact of recent fracture on health-related quality of life in postmenopausal women. J Bone Miner Res. 2006;21(6): 809-816. - PubMed
-
- Hallberg I, Rosenqvist AM, Kartous L, Lofman O, Wahlstrom O, Toss G. Health-related quality of life after osteoporotic fractures. Osteoporos Int. 2004;15(10):834-841. - PubMed
-
- Morin S, Lix LM, Azimaee M, Metge C, Caetano P, Leslie WD. Mortality rates after incident non-traumatic fractures in older men and women. Osteoporos Int. 2011;22(9):2439-2448. - PubMed
-
- Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res. 2007;22(3):465-475. - PubMed
-
- et al. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009;(113):S1-130. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
