

Cell-free human papillomavirus DNA kinetics after surgery for human papillomavirus-associated oropharyngeal cancer
- PMID: 35139236
- PMCID: PMC10032347
- DOI: 10.1002/cncr.34109
Cell-free human papillomavirus DNA kinetics after surgery for human papillomavirus-associated oropharyngeal cancer
Abstract
Background: New ultrasensitive methods for detecting residual disease after surgery are needed in human papillomavirus-associated oropharyngeal squamous cell carcinoma (HPV+OPSCC).
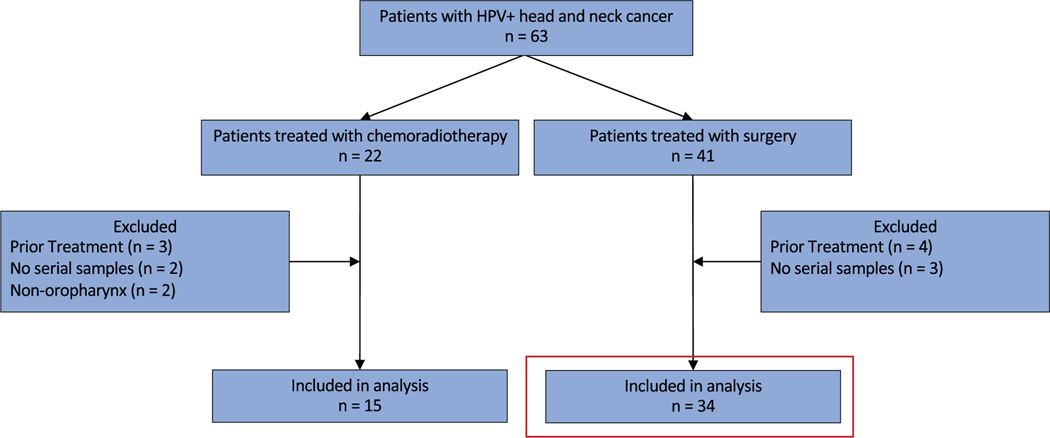
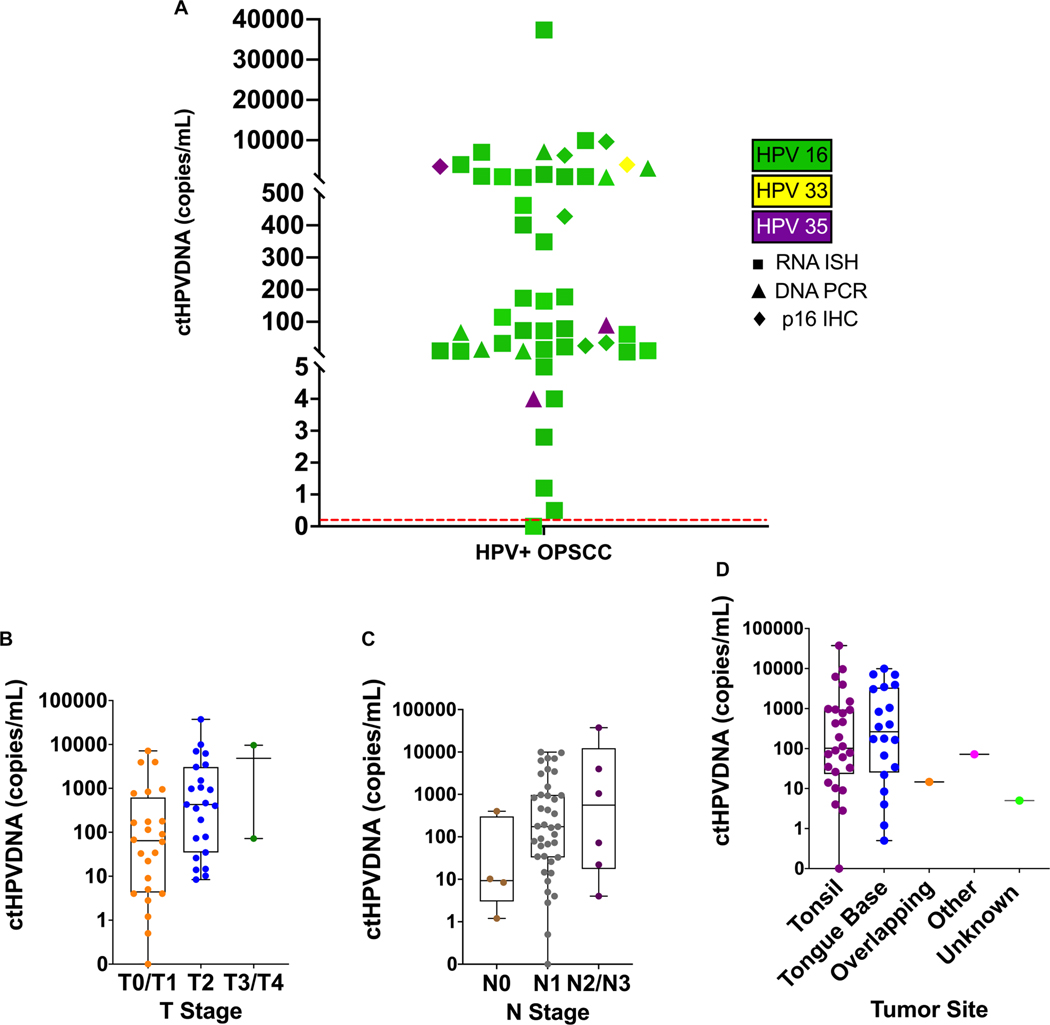
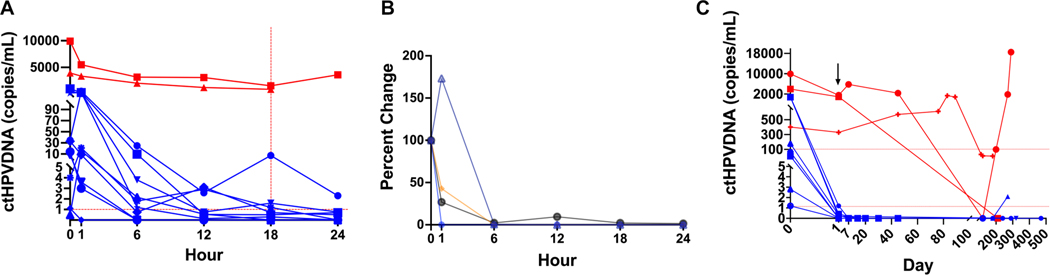
Methods: To determine whether the clearance kinetics of circulating tumor human papillomavirus DNA (ctHPVDNA) is associated with postoperative disease status, a prospective observational study was conducted in 33 patients with HPV+OPSCC undergoing surgery. Blood was collected before surgery, postoperative days 1 (POD 1), 7, and 30 and with follow-up. A subcohort of 12 patients underwent frequent blood collections in the first 24 hours after surgery to define early clearance kinetics. Plasma was run on custom droplet digital polymerase chain reaction (ddPCR) assays for HPV genotypes 16, 18, 33, 35, and 45.
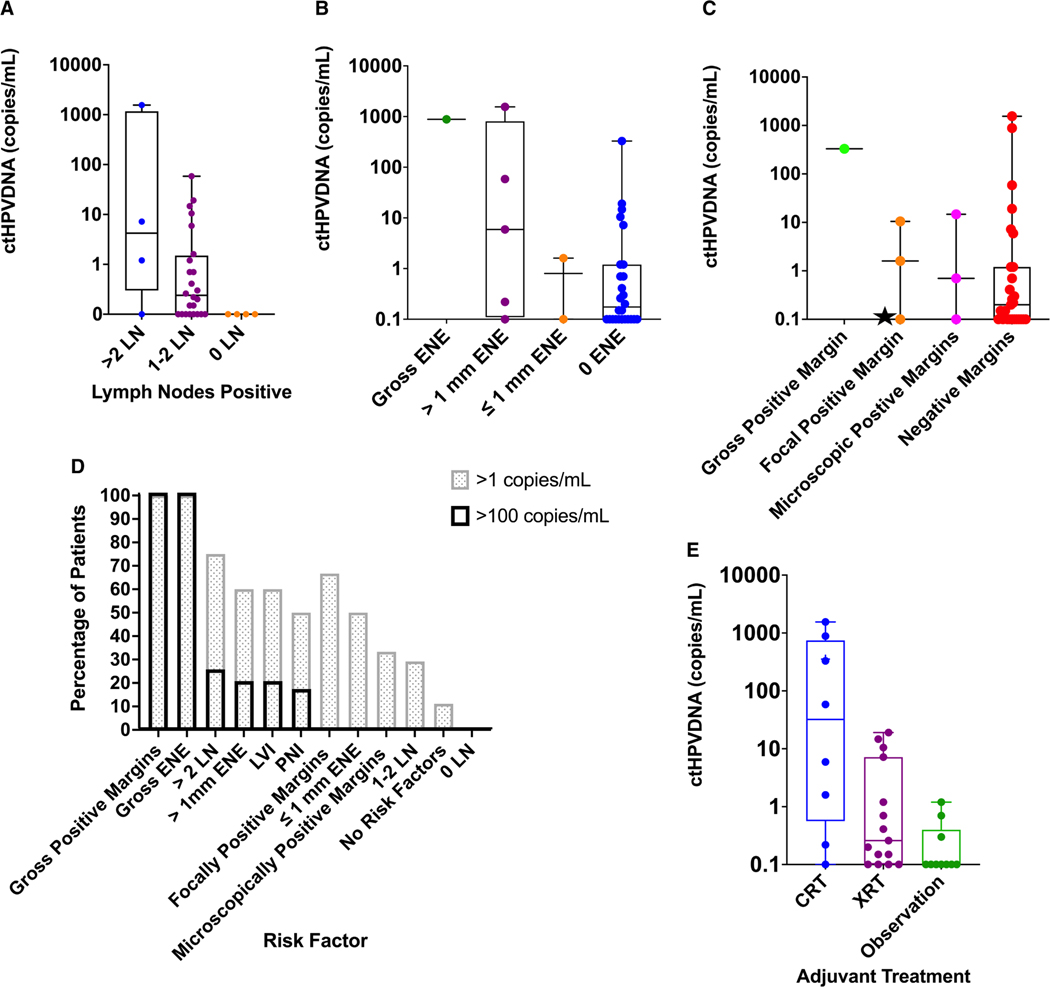
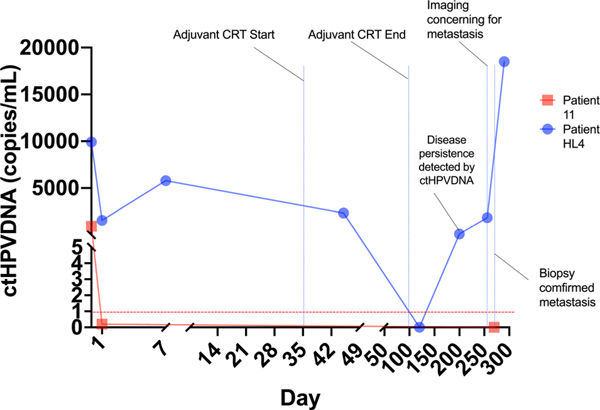
Results: In patients without pathologic risk factors for recurrence who were observed after surgery, ctHPVDNA rapidly decreased to <1 copy/mL by POD 1 (n = 8/8). In patients with risk factors for macroscopic residual disease, ctHPVDNA was markedly elevated on POD 1 (>350 copies/mL) and remained elevated until adjuvant treatment (n = 3/3). Patients with intermediate POD 1 ctHPVDNA levels (1.2-58.4 copies/mL) all possessed pathologic risk factors for microscopic residual disease (n = 9/9). POD 1 ctHPVDNA levels were higher in patients with known adverse pathologic risk factors such as extranodal extension >1 mm (P = .0481) and with increasing lymph nodes involved (P = .0453) and were further associated with adjuvant treatment received (P = .0076). One of 33 patients had a recurrence that was detected by ctHPVDNA 2 months earlier than clinical detection.
Conclusions: POD 1 ctHPVDNA levels are associated with the risk of residual disease in patients with HPV+OPSCC undergoing curative intent surgery and thus could be used as a personalized biomarker for selecting adjuvant treatment in the future.
Lay summary: Human papillomavirus-associated oropharyngeal squamous cell carcinoma (HPV+OPSCC) is increasing at epidemic proportions and is commonly treated with surgery. This report describes results from a study examining the clearance kinetics of circulating tumor HPV DNA (circulating tumor human papillomavirus DNA [ctHPVDNA]) following surgical treatment of HPV+OPSCC. We found that ctHPVDNA levels 1 day after surgery are associated with the risk of residual disease in patients with HPV+OPSCC and thus could be used as a personalized biomarker for selecting adjuvant treatment in the future. These findings are the first to demonstrate the potential utility of ctHPVDNA in patients with HPV+OPSCC undergoing surgery.
Keywords: cell-free DNA; circulating tumor DNA; head and neck cancer; human papillomavirus (HPV); oropharyngeal cancer.
© 2022 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
The other authors made no disclosures.
Figures
Comment in
-
Circulating tumor DNA in head and neck cancer: Early successes and future promise.Cancer. 2022 Jun 1;128(11):2061-2063. doi: 10.1002/cncr.34189. Epub 2022 Mar 17. Cancer. 2022. PMID: 35298053
References
-
- Number of HPV-associated cancer cases per year. Centers for Disease Control and Prevention. Updated August 2, 2019. Accessed May 19–20, 2020. https://www.cdc.gov/cancer/hpv/statistics/cases.htm
-
- Tota JE, Best AF, Zumsteg ZS, Gillison ML, Rosenberg PS, Chaturvedi AK. Evolution of the oropharynx cancer epidemic in the United States: moderation of increasing incidence in younger individuals and shift in the burden to older individuals. J Clin Oncol. 2019;37:1538–1546. doi:10.1200/jco.19.00370 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
