

Cortical microstructure in primary progressive aphasia: a multicenter study
- PMID: 35139897
- PMCID: PMC8830043
- DOI: 10.1186/s13195-022-00974-0
Cortical microstructure in primary progressive aphasia: a multicenter study
Erratum in
-
Correction: Cortical microstructure in primary progressive aphasia: a multicenter study.Alzheimers Res Ther. 2023 Feb 4;15(1):29. doi: 10.1186/s13195-023-01179-9. Alzheimers Res Ther. 2023. PMID: 36739431 Free PMC article. No abstract available.
Abstract
Background: Cortical mean diffusivity is a novel imaging metric sensitive to early changes in neurodegenerative syndromes. Higher cortical mean diffusivity values reflect microstructural disorganization and have been proposed as a sensitive biomarker that might antedate macroscopic cortical changes. We aimed to test the hypothesis that cortical mean diffusivity is more sensitive than cortical thickness to detect cortical changes in primary progressive aphasia (PPA).
Methods: In this multicenter, case-control study, we recruited 120 patients with PPA (52 non-fluent, 31 semantic, and 32 logopenic variants; and 5 GRN-related PPA) as well as 89 controls from three centers. The 3-Tesla MRI protocol included structural and diffusion-weighted sequences. Disease severity was assessed with the Clinical Dementia Rating scale. Cortical thickness and cortical mean diffusivity were computed using a surface-based approach.
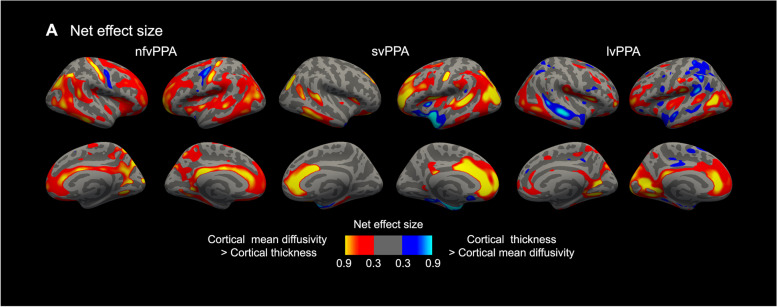
Results: The comparison between each PPA variant and controls revealed cortical mean diffusivity increases and cortical thinning in overlapping regions, reflecting the canonical loci of neurodegeneration of each variant. Importantly, cortical mean diffusivity increases also expanded to other PPA-related areas and correlated with disease severity in all PPA groups. Cortical mean diffusivity was also increased in patients with very mild PPA when only minimal cortical thinning was observed and showed a good correlation with measures of disease severity.
Conclusions: Cortical mean diffusivity shows promise as a sensitive biomarker for the study of the neurodegeneration-related microstructural changes in PPA.
Keywords: Alzheimer’s disease; Diffusion; Frontotemporal lobar degeneration; Magnetic resonance; Primary progressive aphasia.
© 2022. The Author(s).
Conflict of interest statement
I.I.G. reports no disclosures; V.M. reports no disclosures; S.B.E. reports no disclosures; M.L.M. reports no disclosures; N.F. reports no disclosures; A.E.W reports no disclosures; J.P. received an award from the Spanish Society of Neurology (best communication award); M.S.S reports no disclosures; A.B. was awarded in 2019 with the travel Fellowship from the Alzheimer’s Association to attend to the Alzheimer’s Association International Conference (AAIC); D.A. has a patent (WO2019175379 A1 Markers of synaptopathy in neurodegenerative disease) and participated in advisory boards from Fujirebio-Europe and Roche Diagnostics and speaker honoraria from Fujirebio-Europe, Roche Diagnostics, Nutricia, Krka Farmacéutica S.L., Zambon S.A.U., and Esteve Pharmaceuticals S.A; O.D.I reports no disclosures; O.B. has a patent (WO2019175379 A1 markers of synaptopathy in neurodegenerative disease); B.S.S. reports no disclosures; N.B. is member of the executive committee of the European Society of Radiology and reports examiner honoraria from the European Board of Neuroradiology; S.G.O. reports no disclosures; A. Llado reports no disclosures; R.B. reports honoraria from Nutricia; B.C.D reports no disclosures; H.J.R. reports honoraria from Biogen, Wave neuroscience, and Ionis; B.L.M. reports honoraria from Biogen, Cambridge University Press Guilford Publications, Inc. Oxford University Press Taylor & Francis Group Elsevier, Inc.; B.L.M. also served as medical/scientific advisor of The John Douglas French Foundation, The Larry L. Hillblom Foundation, Association for Frontotemporal Degeneration, National Institute for Health Research Cambridge Biomedical Research Centre and its subunit, the Biomedical Research Unit in Dementia, University of Washington ADRC, Stanford University ADRC, Arizona Alzheimer’s Disease Center (ADC), Massachusetts Alzheimer Disease Research Center, The Buck Institute for Research on Aging, University of Southern California (USC) PO1 Urban Air Pollution and Alzheimer’s Disease: Risk, Heterogeneity and Mechanisms. A.Lleó has a patent (WO2019175379 A1 Markers of synaptopathy in neurodegenerative disease); received personal consulting fees from Biogen, Nutricia, Roche, and Fujirebio-Europe; and has served at scientific advisory boards from Fujirebio-Europe, Nutricia, Biogen, and Roche Diagnostics and has filed a patent application of synaptic markers in neurodegenerative diseases; M.G.T. reports no disclosures; R.S.V. has served at scientific advisory boards from Wave pharmaceuticals and Ionis-Biogen and received personal honoraria from Janssen, Roche Diagnostics, Neuraxpharm for educational activities; D.C.P. reports no disclosures; J.F. has a patent (WO2019175379 A1 Markers of synaptopathy in neurodegenerative disease), has served at advisory boards for AC Immune, Zambon, and Lundbeck, and received honoraria for lectures from Roche, NovoNordisk, Esteve, and Biogen.
Figures





References
-
- Mesulam MM. Primary progressive aphasia. Ann Neurol. 2001;49:425–432. - PubMed
