

Risk of persistent and new clinical sequelae among adults aged 65 years and older during the post-acute phase of SARS-CoV-2 infection: retrospective cohort study
- PMID: 35140117
- PMCID: PMC8828141
- DOI: 10.1136/bmj-2021-068414
Risk of persistent and new clinical sequelae among adults aged 65 years and older during the post-acute phase of SARS-CoV-2 infection: retrospective cohort study
Abstract
Objective: To characterize the risk of persistent and new clinical sequelae in adults aged ≥65 years after the acute phase of SARS-CoV-2 infection.
Design: Retrospective cohort study.
Setting: UnitedHealth Group Clinical Research Database: deidentified administrative claims and outpatient laboratory test results.
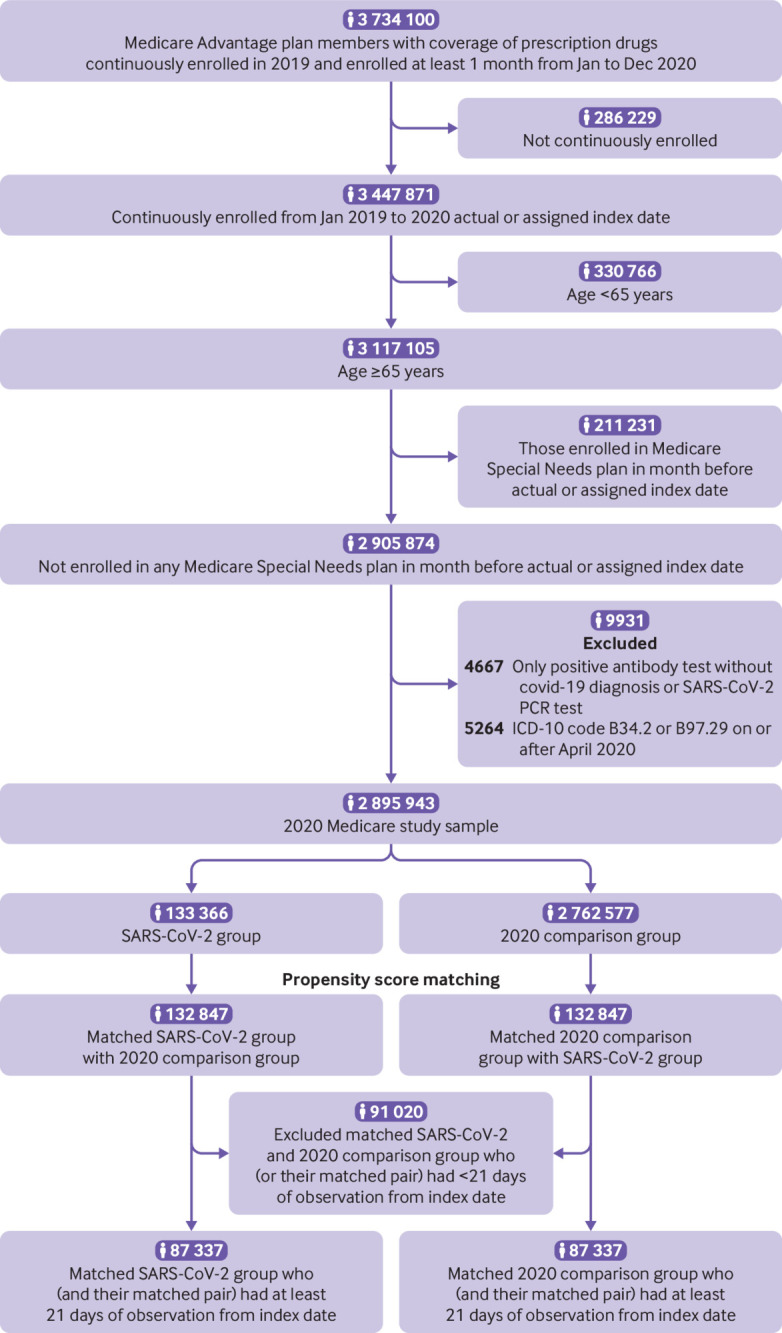
Participants: Individuals aged ≥65 years who were continuously enrolled in a Medicare Advantage plan with coverage of prescription drugs from January 2019 to the date of diagnosis of SARS-CoV-2 infection, matched by propensity score to three comparison groups that did not have covid-19: 2020 comparison group (n=87 337), historical 2019 comparison group (n=88 070), and historical comparison group with viral lower respiratory tract illness (n=73 490).
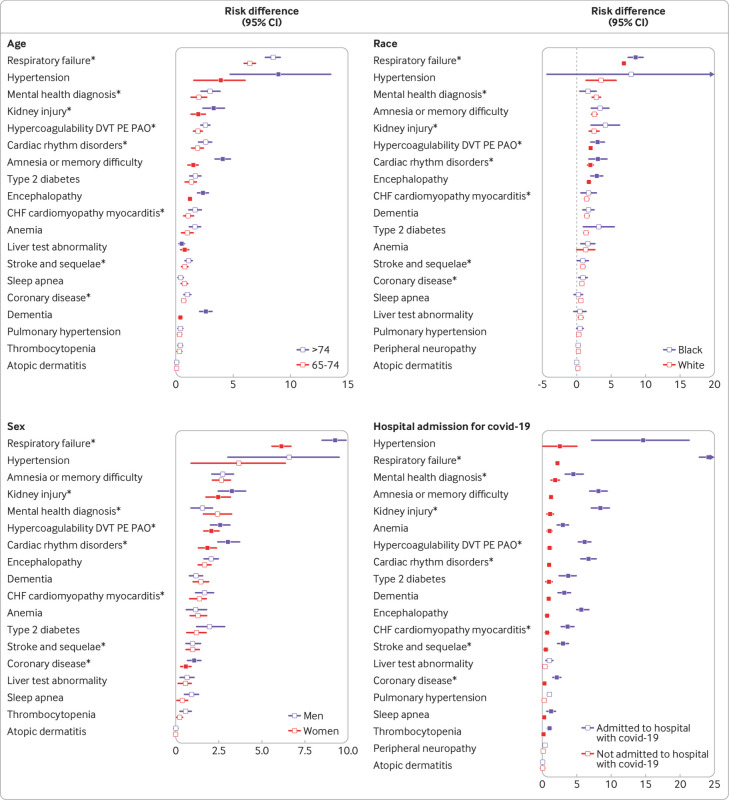
Main outcome measures: The presence of persistent and new sequelae at 21 or more days after a diagnosis of covid-19 was determined with ICD-10 (international classification of diseases, 10th revision) codes. Excess risk for sequelae caused by infection with SARS-CoV-2 was estimated for the 120 days after the acute phase of the illness with risk difference and hazard ratios, calculated with 95% Bonferroni corrected confidence intervals. The incidence of sequelae after the acute infection was analyzed by age, race, sex, and whether patients were admitted to hospital for covid-19.
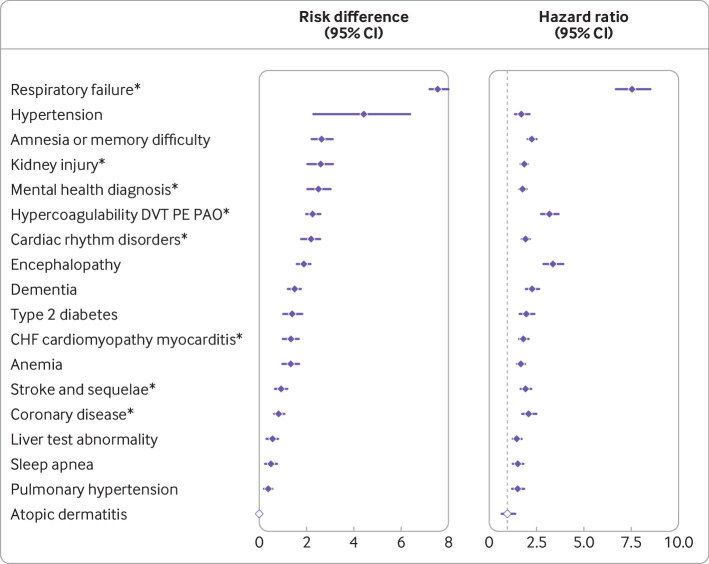
Results: Among individuals who were diagnosed with SARS-CoV-2, 32% (27 698 of 87 337) sought medical attention in the post-acute period for one or more new or persistent clinical sequelae, which was 11% higher than the 2020 comparison group. Respiratory failure (risk difference 7.55, 95% confidence interval 7.18 to 8.01), fatigue (5.66, 5.03 to 6.27), hypertension (4.43, 2.27 to 6.37), memory difficulties (2.63, 2.23 to 3.13), kidney injury (2.59, 2.03 to 3.12), mental health diagnoses (2.50, 2.04 to 3.04), hypercoagulability 1.47 (1.2 to 1.73), and cardiac rhythm disorders (2.19, 1.76 to 2.57) had the greatest risk differences compared with the 2020 comparison group, with similar findings to the 2019 comparison group. Compared with the group with viral lower respiratory tract illness, however, only respiratory failure, dementia, and post-viral fatigue had increased risk differences of 2.39 (95% confidence interval 1.79 to 2.94), 0.71 (0.3 to 1.08), and 0.18 (0.11 to 0.26) per 100 patients, respectively. Individuals with severe covid-19 disease requiring admission to hospital had a markedly increased risk for most but not all clinical sequelae.
Conclusions: The results confirm an excess risk for persistent and new sequelae in adults aged ≥65 years after acute infection with SARS-CoV-2. Other than respiratory failure, dementia, and post-viral fatigue, the sequelae resembled those of viral lower respiratory tract illness in older adults. These findings further highlight the wide range of important sequelae after acute infection with the SARS-CoV-2 virus.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from Optum Laboratories for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. KC declares consulting from Pfizer. ML declares honoraria/consulting from Merck, Sanofi-Pasteur, Bristol Myers-Squibb, and Antigen Discovery; research funding (institutional) from Pfizer; and unpaid scientific advisory services to Janssen, Astra-Zeneca, One Day Sooner, and Covaxx (United Biomedical).
Figures
References
-
- Dennis A, Wamil M, Kapur S, et al. Multi-organ impairment in low-risk individuals with long COVID. bioRxiv. 2020. 10.1101/2020.10.14.20212555 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous