Evidence that large vessels do affect near infrared spectroscopy
- PMID: 35140261
- PMCID: PMC8828816
- DOI: 10.1038/s41598-022-05863-y
Evidence that large vessels do affect near infrared spectroscopy
Abstract
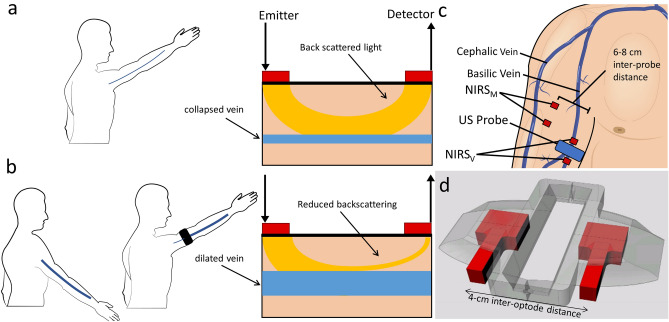
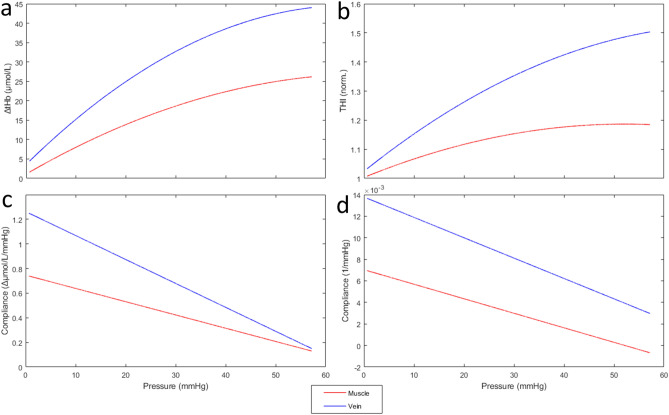
The influence of large vessels on near infrared spectroscopy (NIRS) measurement is generally considered negligible. Aim of this study is to test the hypothesis that changes in the vessel size, by varying the amount of absorbed NIR light, could profoundly affect NIRS blood volume indexes. Changes in haemoglobin concentration (tHb) and in tissue haemoglobin index (THI) were monitored over the basilic vein (BV) and over the biceps muscle belly, in 11 subjects (7 M - 4 F; age 31 ± 8 year) with simultaneous ultrasound monitoring of BV size. The arm was subjected to venous occlusion, according to two pressure profiles: slow (from 0 to 60 mmHg in 135 s) and rapid (0 to 40 mmHg maintained for 30 s). Both tHb and THI detected a larger blood volume increase (1.7 to 4 fold; p < 0.01) and exhibited a faster increase and a greater convexity on the BV than on the muscle. In addition, NIRS signals from BV exhibited higher correlation with changes in BV size than from muscle (r = 0.91 vs 0.55, p < 0.001 for THI). A collection of individual relevant recordings is also included. These results challenge the long-standing belief that the NIRS measurement is unaffected by large vessels and support the concept that large veins may be a major determinant of blood volume changes in multiple experimental conditions.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures