

Limitations of Gravimetric Quantitative Blood Loss during Cesarean Delivery
- PMID: 35141034
- PMCID: PMC8816625
- DOI: 10.1055/s-0041-1742267
Limitations of Gravimetric Quantitative Blood Loss during Cesarean Delivery
Abstract
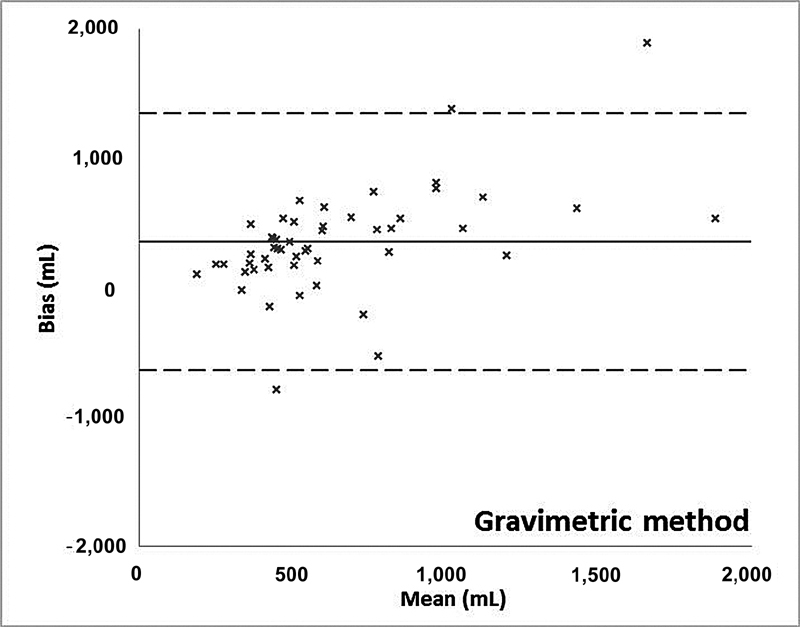
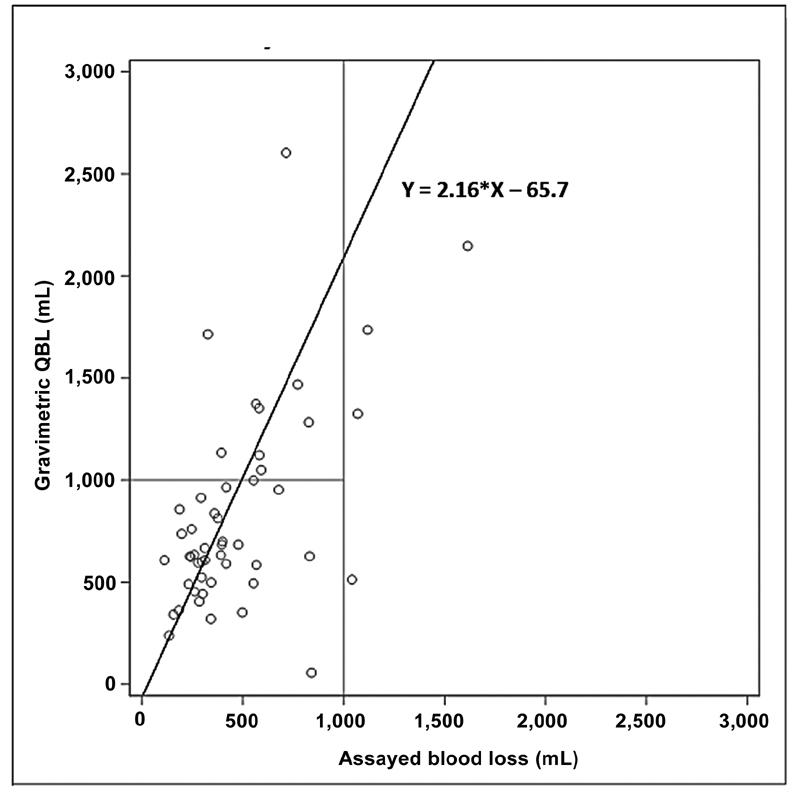
Objective This study examined the accuracy, sources of error, and limitations of gravimetric quantification of blood loss (QBL) during cesarean delivery. Study Design Blood loss determined by assays of the hemoglobin content on surgical sponges and in suction canisters was compared with QBL in 50 parturients. Results QBL was moderately correlated to the actual blood loss ( r = 0.564; p < 0.001). Compared with the reference assay, QBL overestimated blood loss for 44 patients (88%). QBL deviated from the assayed blood loss by more than 250 mL in 34 patients (68%) and by more than 500 mL in 16 cases (32%). Assayed blood loss was more than 1,000 mL in four patients. For three of these patients, QBL was more than 1,000 mL (sensitivity = 75%). QBL was more than 1,000 mL in 12 patients. While three of these had an assayed blood loss of more than 1,000 mL, 9 of the 46 patients with blood losses of less than 1,000 mL by the assay (20%) were incorrectly identified as having postpartum hemorrhage by QBL (false positives). The specificity of quantitative QBL for detection of blood loss more than or equal to 1,000 mL was 80.4%. Conclusion QBL was only moderately correlated with the reference assay. While overestimation was more common than underestimation, both occurred. Moreover, QBL was particularly inaccurate when substantial bleeding occurred. Key Points QBL is inaccurate in cesarean delivery.QBL deviated from the assay result by more than 500 mL in 32% of cases.QBL sensitivity and specificity for hemorrhage is 75.0% (95% confidence interval [CI]: 0.19-0.93) and 80.4% (95% CI: 0.69-0.92), respectively.
Keywords: blood loss quantification; cesarean delivery; postpartum hemorrhage; quality improvement.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
Quantitative blood loss after vaginal delivery: a retrospective analysis of 104 079 measurements at 41 institutions.Int J Obstet Anesth. 2022 Aug;51:103256. doi: 10.1016/j.ijoa.2022.103256. Epub 2022 Jan 12. Int J Obstet Anesth. 2022. PMID: 35636143
-
Quantification of Blood Loss Improves Detection of Postpartum Hemorrhage and Accuracy of Postpartum Hemorrhage Rates: A Retrospective Cohort Study.Cureus. 2021 Feb 27;13(2):e13591. doi: 10.7759/cureus.13591. Cureus. 2021. PMID: 33659146 Free PMC article.
-
Impact of measuring quantification of blood loss versus estimation of blood loss during cesarean deliveries.Int J Gynaecol Obstet. 2023 Feb;160(2):670-677. doi: 10.1002/ijgo.14337. Epub 2022 Jul 27. Int J Gynaecol Obstet. 2023. PMID: 35809081
-
Tranexamic acid for the prevention of postpartum hemorrhage in women undergoing cesarean delivery: an updated meta-analysis.Am J Obstet Gynecol. 2022 Apr;226(4):510-523.e22. doi: 10.1016/j.ajog.2021.09.025. Epub 2021 Sep 25. Am J Obstet Gynecol. 2022. PMID: 34582795 Review.
-
Intravenous oxytocin dosing regimens for postpartum hemorrhage prevention following cesarean delivery: a systematic review and meta-analysis.Am J Obstet Gynecol. 2021 Sep;225(3):250.e1-250.e38. doi: 10.1016/j.ajog.2021.04.258. Epub 2021 May 4. Am J Obstet Gynecol. 2021. PMID: 33957113
Cited by
-
Quantitative blood loss values reveal high rates of undiagnosed postpartum hemorrhage.Int J Gynaecol Obstet. 2025 Aug;170(2):614-620. doi: 10.1002/ijgo.70037. Epub 2025 Mar 1. Int J Gynaecol Obstet. 2025. PMID: 40022572 Free PMC article.
References
-
- Quantification of blood loss: AWHONN practice brief number 1. J Obstet Gynecol Neonatal Nurs. 2015;44(01):158–160. - PubMed
-
- Quantitative blood loss in obstetric hemorrhage: ACOG COMMITTEE OPINION, number 794. Obstet Gynecol. 2019;134(06):e150–e156. - PubMed
-
- Main E K, Goffman D, Scavone B M. National Partnership for Maternal Safety: Consensus Bundle on Obstetric Hemorrhage. Obstet Gynecol. 2015;126(01):155–162. - PubMed
-
- Lyndon A, Lagrew D, Shields L E, Main E, Cape V.Improving health care response to obstetric hemorrhage version 2.0Accessed December 16, 2021:https://www.cmqcc.org/resource/obstetric-hemorrhage-20-toolkit
-
- Johar R S, Smith R P. Assessing gravimetric estimation of intraoperative blood loss. J Gynecol Surg. 1993;9(03):151–154. - PubMed
LinkOut - more resources
Full Text Sources