

A Model Predicting Mortality of Hospitalized Covid-19 Patients Four Days After Admission: Development, Internal and Temporal-External Validation
- PMID: 35141170
- PMCID: PMC8819729
- DOI: 10.3389/fcimb.2021.795026
A Model Predicting Mortality of Hospitalized Covid-19 Patients Four Days After Admission: Development, Internal and Temporal-External Validation
Abstract
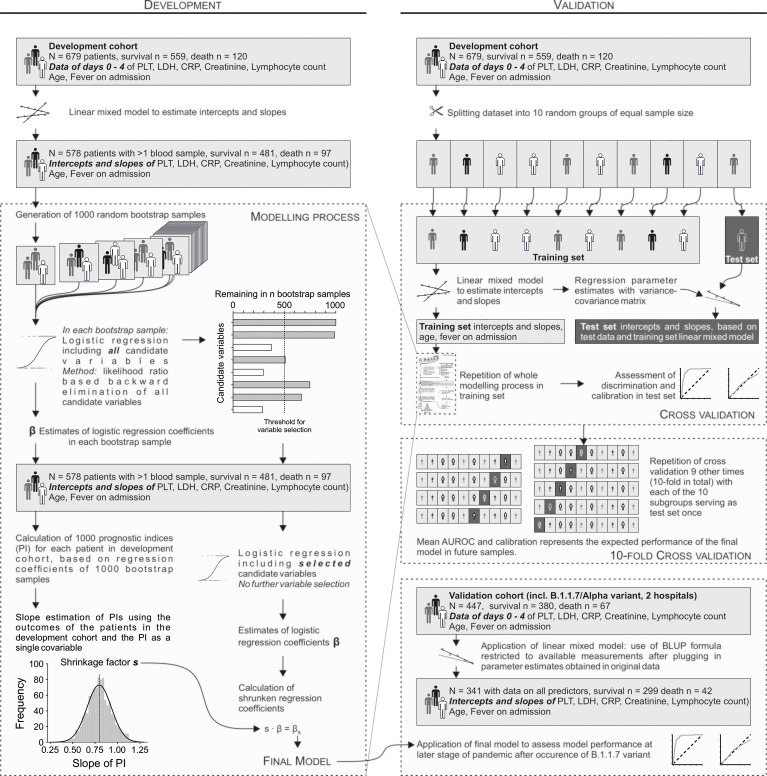
Objective: To develop and validate a prognostic model for in-hospital mortality after four days based on age, fever at admission and five haematological parameters routinely measured in hospitalized Covid-19 patients during the first four days after admission.
Methods: Haematological parameters measured during the first 4 days after admission were subjected to a linear mixed model to obtain patient-specific intercepts and slopes for each parameter. A prediction model was built using logistic regression with variable selection and shrinkage factor estimation supported by bootstrapping. Model development was based on 481 survivors and 97 non-survivors, hospitalized before the occurrence of mutations. Internal validation was done by 10-fold cross-validation. The model was temporally-externally validated in 299 survivors and 42 non-survivors hospitalized when the Alpha variant (B.1.1.7) was prevalent.
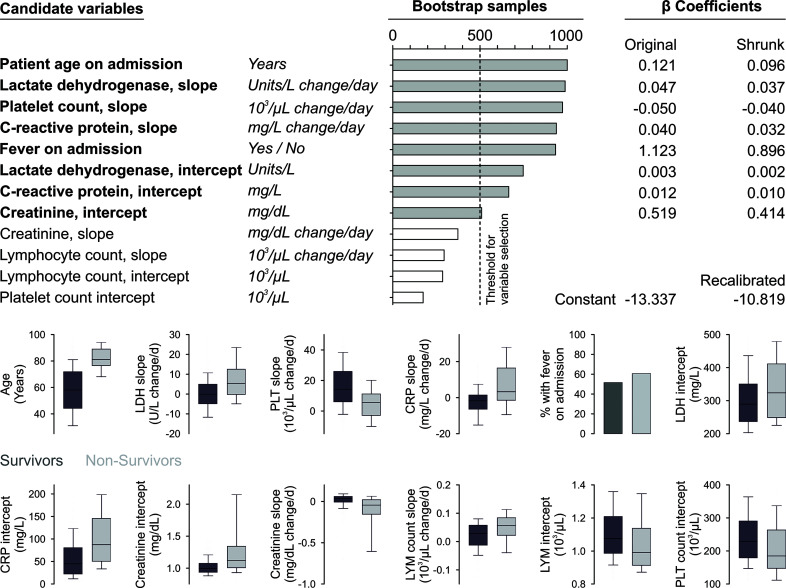
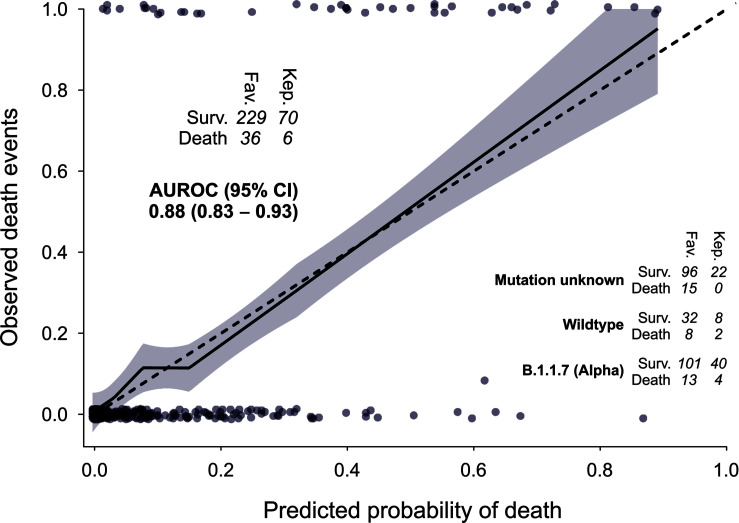
Results: The final model included age, fever on admission as well as the slope or intercept of lactate dehydrogenase, platelet count, C-reactive protein, and creatinine. Tenfold cross validation resulted in a mean area under the receiver operating characteristic curve (AUROC) of 0.92, a mean calibration slope of 1.0023 and a Brier score of 0.076. At temporal-external validation, application of the previously developed model showed an AUROC of 0.88, a calibration slope of 0.95 and a Brier score of 0.073. Regarding the relative importance of the variables, the (apparent) variation in mortality explained by the six variables deduced from the haematological parameters measured during the first four days is higher (explained variation 0.295) than that of age (0.210).
Conclusions: The presented model requires only variables routinely acquired in hospitals, which allows immediate and wide-spread use as a decision support for earlier discharge of low-risk patients to reduce the burden on the health care system.
Clinical trial registration: Austrian Coronavirus Adaptive Clinical Trial (ACOVACT); ClinicalTrials.gov, identifier NCT04351724.
Keywords: COVID-19; blood parameter; hospitalized patients; logistic regression; prediction model; survival.
Copyright © 2022 Heber, Pereyra, Schrottmaier, Kammerer, Santol, Rumpf, Pawelka, Hanna, Scholz, Liu, Hell, Heiplik, Lickefett, Havervall, Traugott, Neuböck, Schörgenhofer, Seitz, Firbas, Karolyi, Weiss, Jilma, Thålin, Bellmann-Weiler, Salzer, Szepannek, Fischer, Zoufaly, Gleiss and Assinger.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Apley D. W., Zhu J. (2020). Visualizing the Effects of Predictor Variables in Black Box Supervised Learning Models. J. R. Stat. Soc.: Ser. B (Stat. Method) 82 (4), 1059–1086. doi: 10.1111/rssb.12377 - DOI
-
- Bücker M., Szepannek G., Gosiewska A., Biecek P. (2021). Transparency, Auditability, and Explainability of Machine Learning Models in Credit Scoring. J. Oper. Res. Soc. 1–21. doi: 10.1080/01605682.2021.1922098 - DOI
Publication types
MeSH terms
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials