

Short-segment minimally disruptive anterior column release for focal sagittal deformity correction of the thoracolumbar spine
- PMID: 35141633
- PMCID: PMC8820079
- DOI: 10.1016/j.xnsj.2021.100068
Short-segment minimally disruptive anterior column release for focal sagittal deformity correction of the thoracolumbar spine
Abstract
Background: Sagittal malalignment is associated with poor quality of life. Correction of lumbar lordosis through anterior column release (ACR) has been shown to improve overall sagittal alignment, however typically in combination with long posterior constructs and associated morbidity. The technical feasibility and radiographic outcomes of short-segment anterior or lateral minimally invasive surgery (MIS) ACR techniques in moderate to severe lumbar sagittal deformity were evaluated.
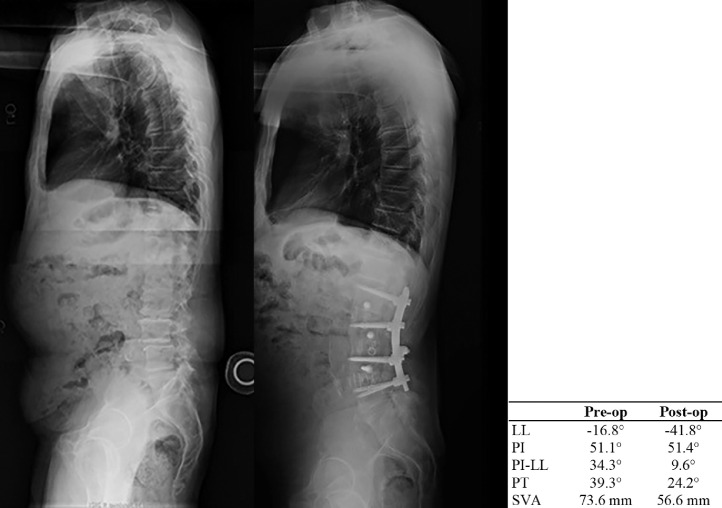
Methods: Consecutive patients treated with short-segment MIS ACR techniques for moderate to severe lumbar sagittal deformity correction were retrospectively analyzed from a prospectively collected database. Clinical outcomes included perioperative measures of invasiveness, including operative time, blood loss, complications, and average length of stay. Radiographic outcomes included measurement of preoperative, immediate postoperative, and long-term follow-up radiographic parameters including coronal Cobb angle, lumbar lordosis (LL), pelvic incidence (PI), PI-LL mismatch, pelvic tilt (PT), T1 pelvic angle (TPA), T1 spino-pelvic inclination (T1SPI), proximal junctional angle (PJA), and sagittal vertical axis (SVA).
Results: The cohort included 34 patients (mean age 63) who were treated at an average 2.5 interbody levels (range 1-4) through a lateral or anterior approach (LLIF or ALIF). Of 89 total interbody levels treated, 63 (71%) were ACR levels. Posterior fixation was across an average of 3.2 levels (range 1-5). Mean total operative time and blood loss were 362 minutes and 621 mL. Surgical complications occurred in 2 (5.9%). Average hospital stay was 5.5 days (including staging). At last follow-up (average 25.4 months; range 0.5-7 years), all patients (100%) demonstrated successful achievement of one or more alignment goal, with significant improvements in coronal Cobb, LL, PI-LL mismatch, PT, and TPA. No patient was revised for PJK.
Conclusions: These data show that short-segment MIS ACR correction of moderate to severe lumbar sagittal deformity is feasible and effective at achieving overall alignment goals with low procedural morbidity and risk of proximal junctional issues.
Keywords: Anterior column release (ACR); Anterior lumbar interbody fusion (ALIF); Lateral lumbar interbody fusion (LLIF); Minimally invasive surgery (MIS); Proximal junctional kyphosis (PJK); Upper instrumented vertebra (UIV).
© 2021 The Author(s). Published by Elsevier Ltd on behalf of North American Spine Society.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Ozgur B.M., Aryan H.E., Pimenta L., Taylor W.R. Extreme lateral interbody fusion (XLIF): a novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006;6:435–443. - PubMed
-
- Anand N., Baron E.M., Khandehroo B. Limitations and ceiling effects with circumferential minimally invasive correction techniques for adult scoliosis: Analysis of radiological outcomes over a 7-year experience. Neurosurg Focus. 2014;36(5):E14. - PubMed
-
- Yson S.C., Sembrano J.N., Santos E.R., Luna J.T., P.o.l.l.y.D.W. Jr Does prone repositioning before posterior fixation produce greater lordosis in lateral lumbar interbody fusion (LLIF)? J Spinal Disord Tech. 2014;27(7):364–369. - PubMed
-
- Isaacs R.E., Hyde J., Goodrich J.A., Rodgers W.B., Phillips F.M. A prospective, nonrandomized, multicenter evaluation of extreme lateral interbody fusion for the treatment of adult degenerative scoliosis: perioperative outcomes and complications. Spine. 2010;35(26 Suppl):S322–S330. - PubMed
-
- Rodgers W.B., Cox C.S., Gerber E.J. Early complications of extreme lateral interbody fusion in the obese. J Spinal Disord Tech. 2010;23(6):393–397. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
