

doi: 10.1093/icvts/ivac017.
Modified implantation of a Bolton Relay branch arch device into the ascending aorta close to a mechanical aortic valve
Affiliations
- PMID: 35142358
- PMCID: PMC9070509
- DOI: 10.1093/icvts/ivac017
Item in Clipboard
Modified implantation of a Bolton Relay branch arch device into the ascending aorta close to a mechanical aortic valve
Interact Cardiovasc Thorac Surg.
.
Abstract
An aortic arch stent graft is usually contraindicated with a mechanical aortic valve. However, a modified stent graft plus the use of an externalized transapical guidewire technique allowed a safe implantation close to a mechanical aortic valve.
Keywords: Artificial Aortic Valve; Branch Arch Device; Externalized Transapical Guidewire; Physician Modified Endograft.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
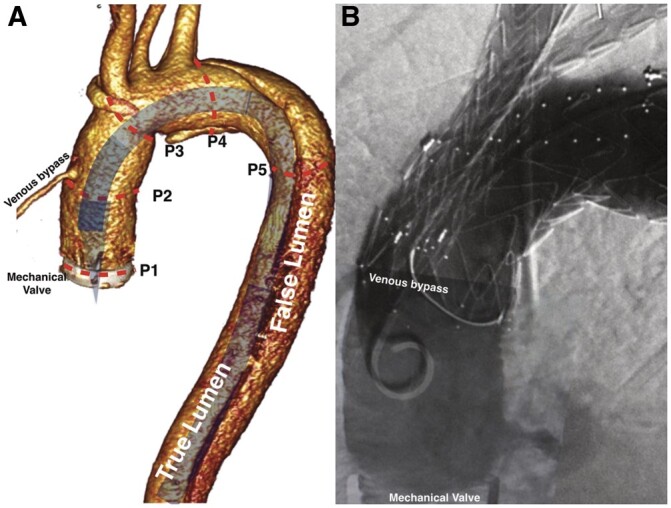
(A) 3-Dimensional reconstruction of the tomographic image. Expected position of a delivery system without tip modification. Sizing: P1–P2: space for the tip of the delivery system (29 mm); P2-P3: proximal sealing zone (34 mm); P3-P4: access to the branches (50 mm); P4-P5: distal sealing zone. (B) Completion angiographic scan: patent venous bypass; no endoleak.
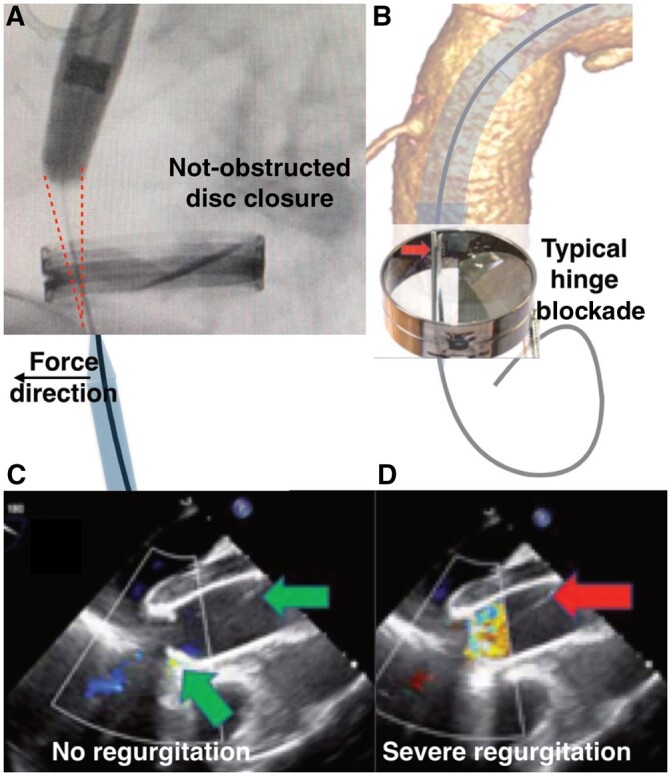
(A) Red sketch on the fluoroscopic image shows space obtained after cutting 15 mm from the tip of the stent graft. The wire was guided by the 6 Fr sheath from the apex to keep it away from the disc hinge. (B) 3-Dimensional reconstruction of the tomographic image. Mechanism of the disc blockade if the valve is simply crossed. (C/D) Transoesophageal echocardiography. (C) Effective valve closure; green arrows show correct position of the wire. (D) Severe valve regurgitation after the blockade of the disc. Red arrow shows the position of the wire.
References
-
- Czerny M, Schmidli J, Adler S, Van Den Berg JC, Bertoglio L, Carrel T, EACTS/ESVS scientific document group et al.Current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic surgery (EACTS) and the European Society for Vascular Surgery (ESVS). Eur J Cardiothorac Surg 2019;55:133–62. - PubMed
-
- Kondov S, Kreibich M, Rylski B, Siepe M, Beyersdorf F, Czerny M.. The endovascular repair of the aortic arch using a double branched prosthesis. J Vis Surg 2018;4:132.
MeSH terms
LinkOut - more resources
Full Text Sources
