

Challenges of imaging interpretation to predict oligodendroglioma grade: a report from the Neuro-Oncology Branch
- PMID: 35142534
- PMCID: PMC8988255
- DOI: 10.2217/cns-2021-0005
Challenges of imaging interpretation to predict oligodendroglioma grade: a report from the Neuro-Oncology Branch
Abstract
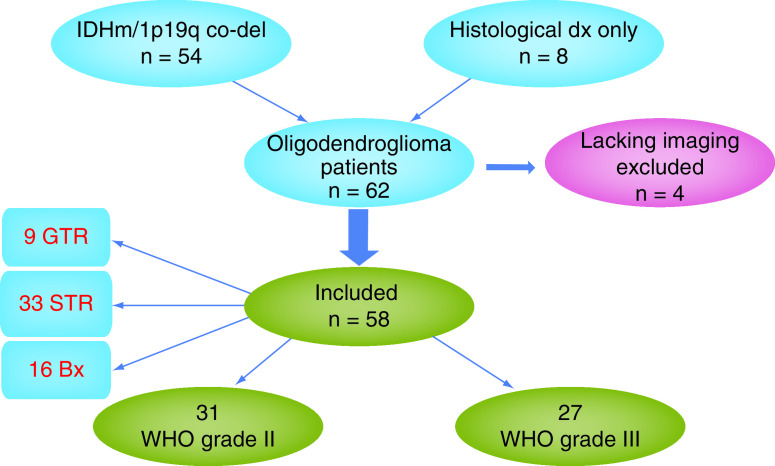
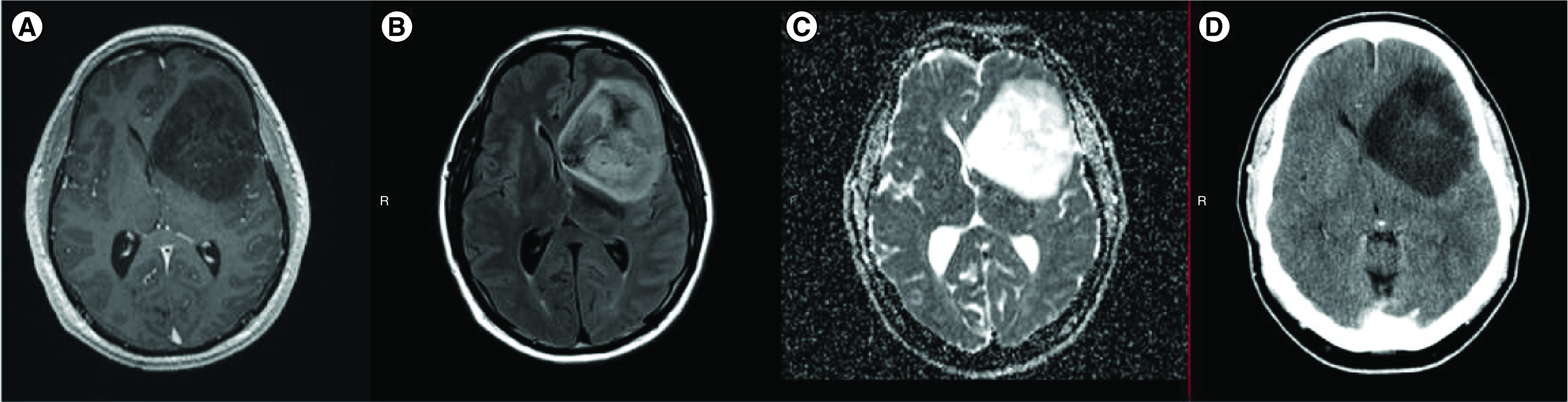
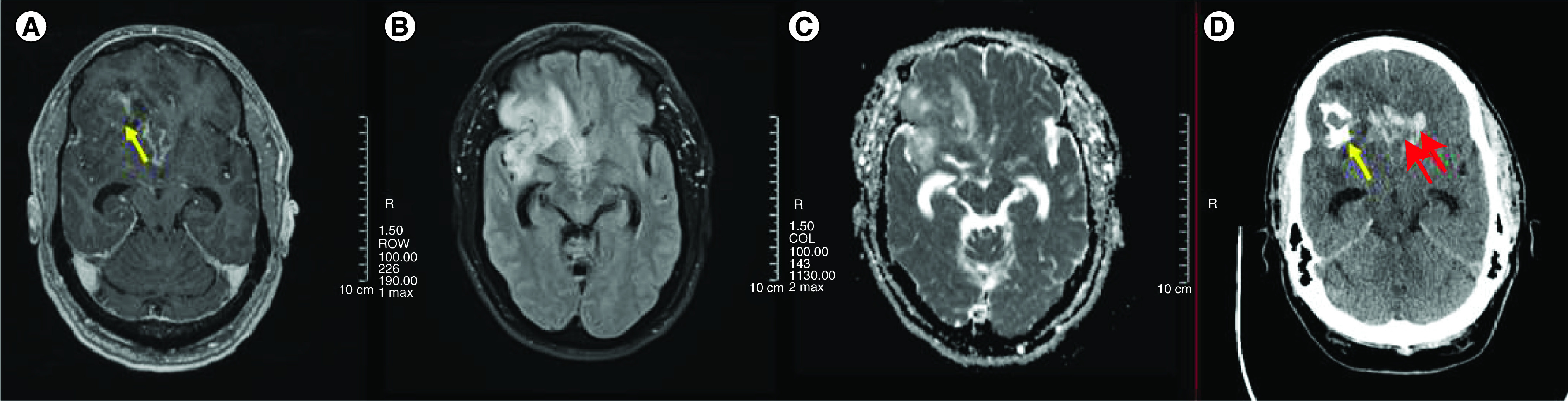
Background: To illustrate challenges of imaging interpretation in patients with oligodendroglioma seen at a referral center and evaluate interrater reliability. Methods: Two neuro-oncologists reviewed diagnostic preradiation MRIs of oligodendroglioma patients; interrater reliability was calculated with the kappa coefficient (k). A neuroradiologist measured presurgical apparent diffusion coefficient (ADC), if available. Results: Extensive enhancement was noted in four of 58 patients, k = 0.7; necrosis in seven of 58, k = 0.61; calcification in seven of 17, k = 1.0; diffusion restriction in two of 39 patients, k = 1.0 (all only in grade 3). ADC values with receiver operator characteristic analysis for area under the curve were 0.473, not significantly different from the null hypothesis (p = 0.14). Conclusions: Extensive enhancement, necrosis and calcification correlated with grade 3 oligodendroglioma in our sample. However, interrater variability is an important limitation when assessing radiographic features, supporting the need for standardization of imaging protocols and their interpretation.
Keywords: calcification; contrast enhancement; examiner concordance; interrater reliability; necrosis; oligodendroglioma; restricted diffusion.
Conflict of interest statement
The authors are members of The NCI Comprehensive Oncology Network for Evaluating Rare CNS Tumors (NCI-CONNECT), which is a program within the Rare Tumor Patient Engagement Network (RTPEN), an initiative supported by the Cancer Moonshot funds and managed at the National Institutes of Health, National Cancer Institute, Center for Cancer Research, Neuro-Oncology Branch. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Figures
References
-
- Penas-Prado M, Wu J, Cahill DP et al. Proceedings of the Comprehensive Oncology Network Evaluating Rare CNS Tumors (NCI-CONNECT) Oligodendroglioma Workshop. Neuro-Oncol. Advances. 2(1), vdz048 (2019). - PMC - PubMed
-
• This article discusses challenges in oligodendroglioma treatment and future directions.
-
- Louis DN, Perry A, Reifenberger G et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta. Neuropathol. 131(6), 803–20 (2016). - PubMed