

A Multicentered Randomized Controlled Trial Comparing the Effectiveness of Pain Treatment Communication Tools in Emergency Department Patients With Back or Kidney Stone Pain
- PMID: 35143273
- PMCID: PMC8842217
- DOI: 10.2105/AJPH.2021.306511
A Multicentered Randomized Controlled Trial Comparing the Effectiveness of Pain Treatment Communication Tools in Emergency Department Patients With Back or Kidney Stone Pain
Abstract
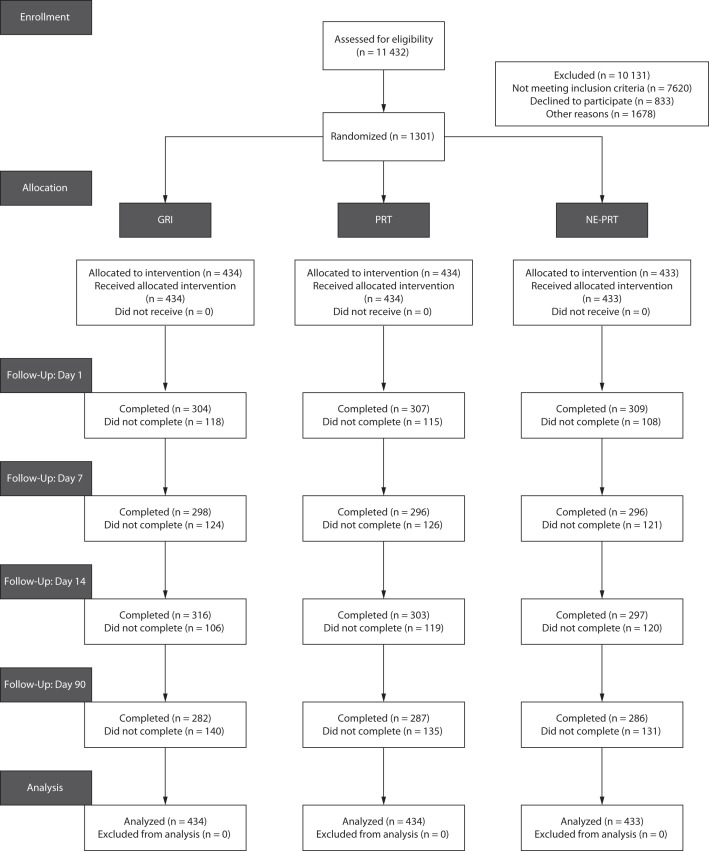
Objectives. To compare the effectiveness of 3 approaches for communicating opioid risk during an emergency department visit for a common painful condition. Methods. This parallel, multicenter randomized controlled trial was conducted at 6 geographically disparate emergency department sites in the United States. Participants included adult patients between 18 and 70 years of age presenting with kidney stone or musculoskeletal back pain. Participants were randomly assigned to 1 of 3 risk communication strategies: (1) a personalized probabilistic risk visual aid, (2) a visual aid and a video narrative, or 3) general risk information. The primary outcomes were accuracy of risk recall, reported opioid use, and treatment preference at time of discharge. Results. A total of 1301 participants were enrolled between June 2017 and August 2019. There was no difference in risk recall at 14 days between the narrative and probabilistic groups (43.7% vs 38.8%; absolute risk reduction = 4.9%; 95% confidence interval [CI] = -2.98, 12.75). The narrative group had lower rates of preference for opioids at discharge than the general risk information group (25.9% vs 33.0%; difference = 7.1%; 95% CI = 0.64, 0.97). There were no differences in reported opioid use at 14 days between the narrative, probabilistic, and general risk groups (10.5%, 10.3%, and 13.3%, respectively; P = .44). Conclusions. An emergency medicine communication tool incorporating probabilistic risk and patient narratives was more effective than general information in mitigating preferences for opioids in the treatment of pain but was not more effective with respect to opioid use or risk recall. Trial Registration. Clinical Trials.gov identifier: NCT03134092. (Am J Public Health. 2022;112(S1):S45-S55. https://doi.org/10.2105/AJPH.2021.306511).
Figures
Comment in
-
Narratives Are Useful Strategies for Overcoming Challenges in Risk Communication.Am J Public Health. 2022 Feb;112(S1):S12-S14. doi: 10.2105/AJPH.2021.306669. Am J Public Health. 2022. PMID: 35143263 Free PMC article. No abstract available.
-
Managing Acute Pain With Opioids in the Emergency Department: A Teachable Moment?Am J Public Health. 2022 Feb;112(S1):S9-S11. doi: 10.2105/AJPH.2022.306748. Am J Public Health. 2022. PMID: 35143264 Free PMC article. No abstract available.
References
-
- National Institute on Drug Abuse https://www.drugabuse.gov/related-topics/trends-statistics/overdose-deat...2020.
-
- Centers for Disease Control and Prevention. Drug overdose overview. Available https://www.cdc.gov/drugoverdose/data/prescribing/overview.html2020.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
