

Fetal Brain Volume Predicts Neurodevelopment in Congenital Heart Disease
- PMID: 35143287
- PMCID: PMC9007882
- DOI: 10.1161/CIRCULATIONAHA.121.056305
Fetal Brain Volume Predicts Neurodevelopment in Congenital Heart Disease
Abstract
Background: Neurodevelopmental impairment is common in children with congenital heart disease (CHD), but postnatal variables explain only 30% of the variance in outcomes. To explore whether the antecedents for neurodevelopmental disabilities might begin in utero, we analyzed whether fetal brain volume predicted subsequent neurodevelopmental outcome in children with CHD.
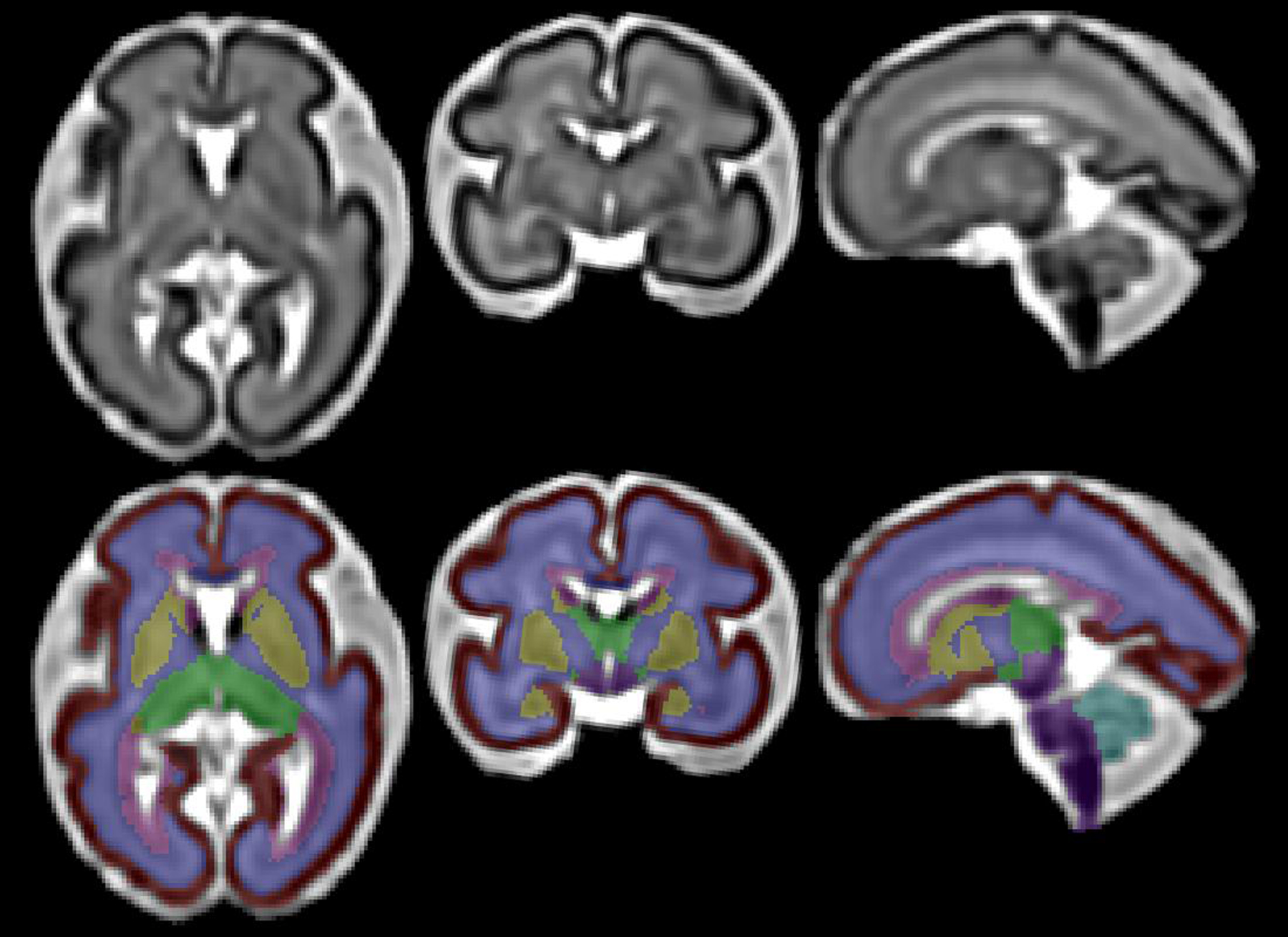
Methods: Fetuses with isolated CHD and sociodemographically comparable healthy control fetuses underwent fetal brain magnetic resonance imaging and 2-year neurodevelopmental evaluation with the Bayley Scales of Infant and Toddler Development, Third Edition (Bayley-III) and the Adaptive Behavior Assessment System, Third Edition (ABAS-3). Hierarchical regression evaluated potential predictors of Bayley-III and ABAS-3 outcomes in the CHD group, including fetal total brain volume adjusted for gestational age and sex, sociodemographic characteristics, birth measures, and medical history.
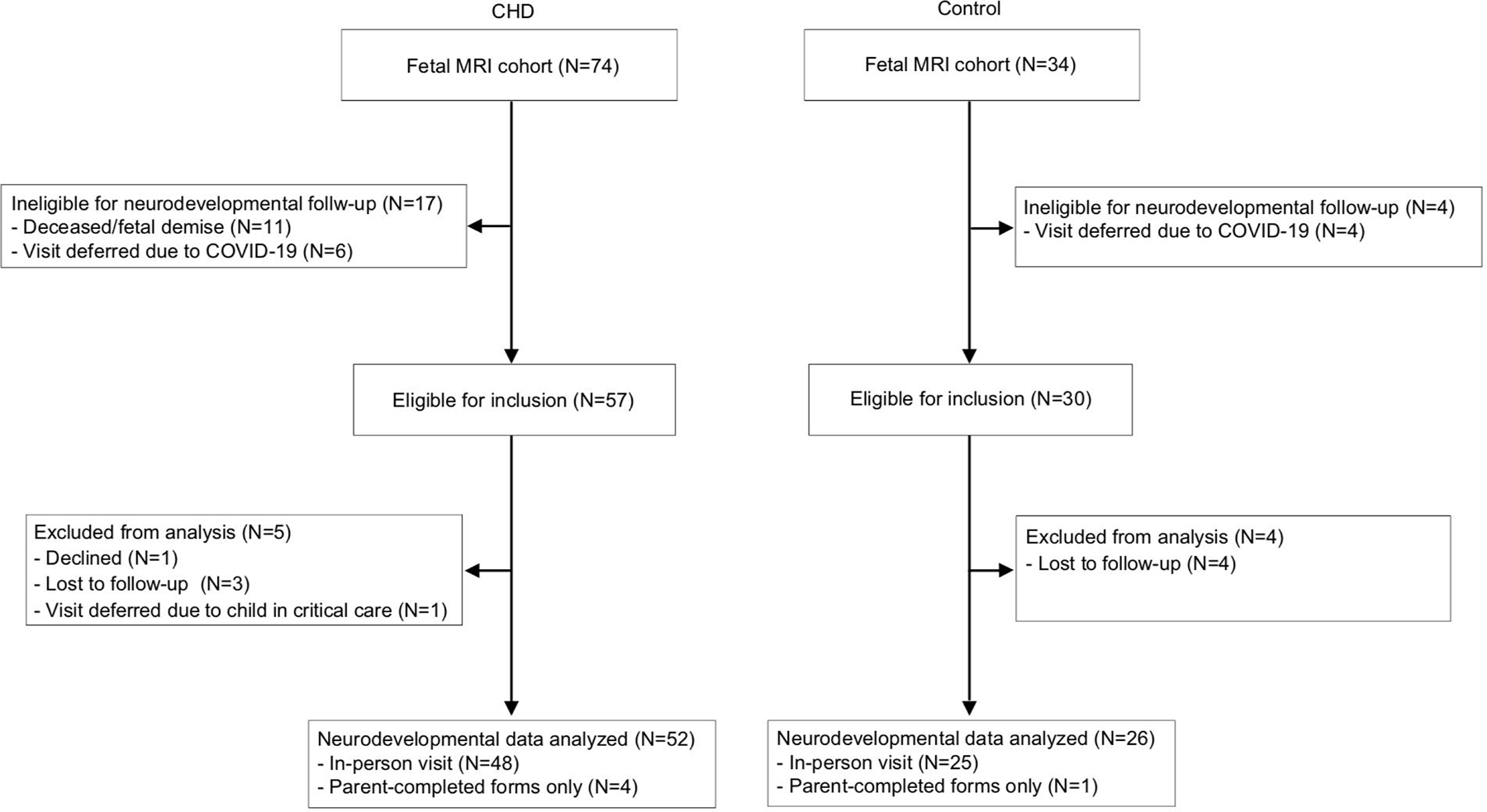
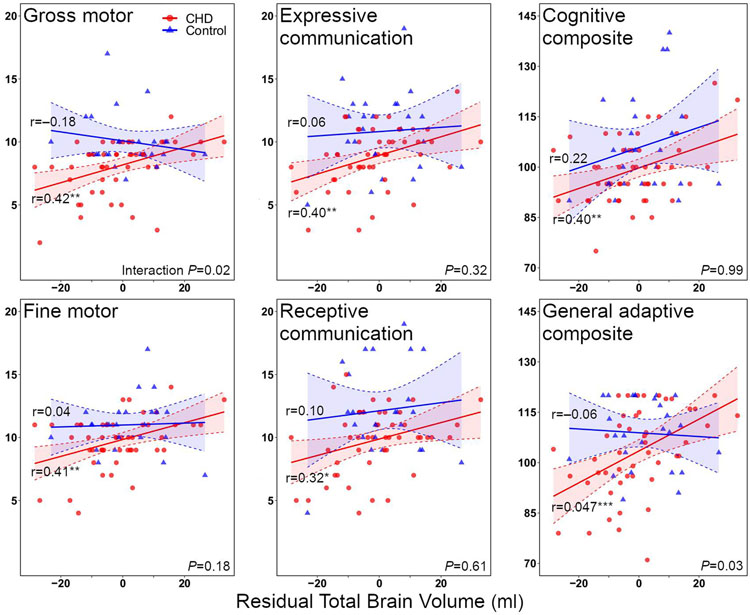
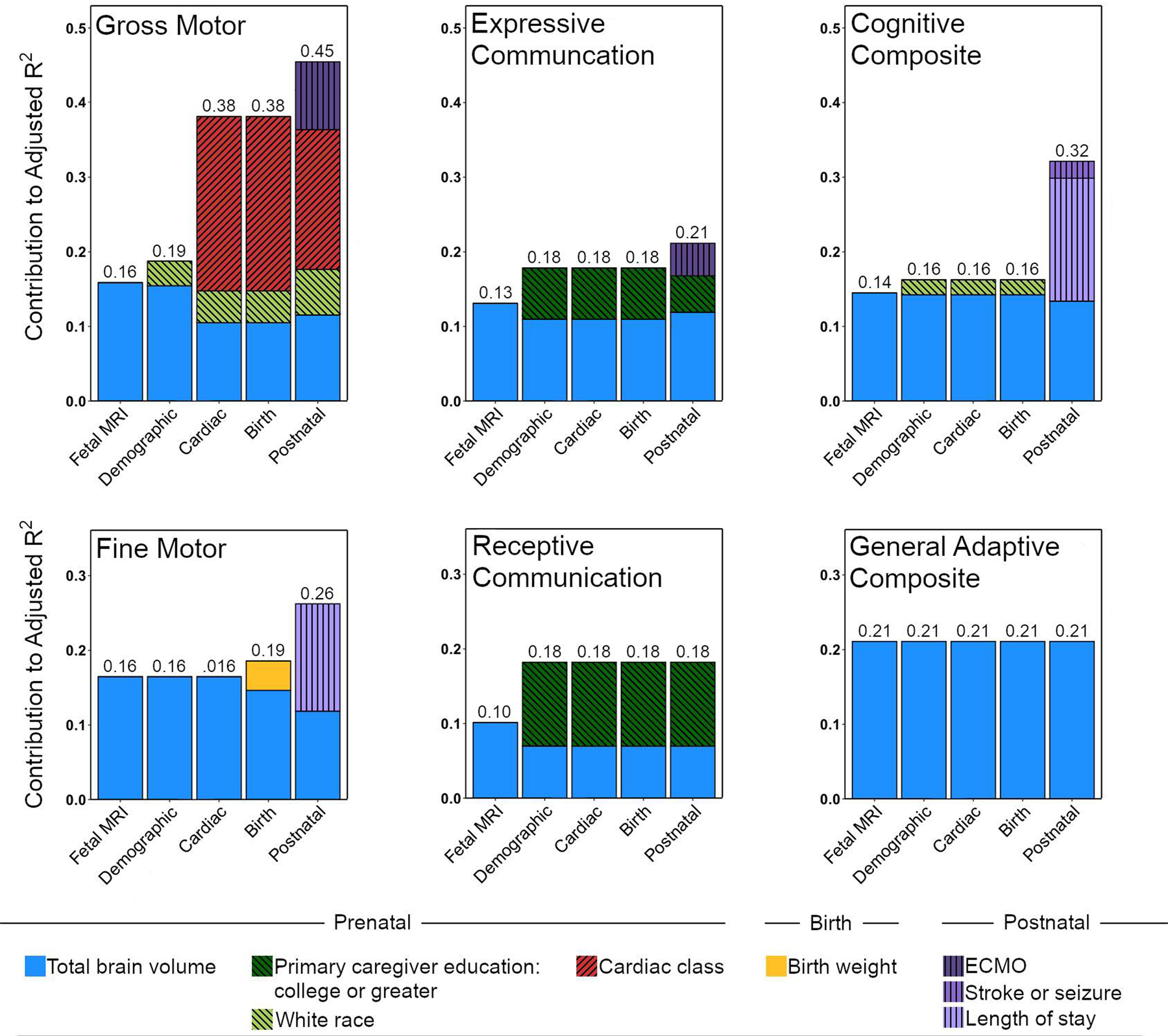
Results: The CHD group (n=52) had lower Bayley-III cognitive, language, and motor scores than the control group (n=26), but fetal brain volumes were similar. Within the CHD group, larger fetal total brain volume correlated with higher Bayley-III cognitive, language, and motor scores and ABAS-3 adaptive functioning scores (r=0.32-0.47; all P<0.05), but this was not noted in the control group. Fetal brain volume predicted 10% to 21% of the variance in neurodevelopmental outcome measures in univariate analyses. Multivariable models that also included social class and postnatal factors explained 18% to 45% of the variance in outcome, depending on developmental domain. Moreover, in final multivariable models, fetal brain volume was the most consistent predictor of neurodevelopmental outcome across domains.
Conclusions: Small fetal brain volume is a strong independent predictor of 2-year neurodevelopmental outcomes and may be an important imaging biomarker of future neurodevelopmental risk in CHD. Future studies are needed to support this hypothesis. Our findings support inclusion of fetal brain volume in risk stratification models and as a possible outcome in fetal neuroprotective intervention studies.
Keywords: brain; heart defects, congenital; magnetic resonance imaging.
Figures
Comment in
-
In Utero Brain Growth Matters for Fetuses With Congenital Heart Disease.Circulation. 2022 Apr 12;145(15):1120-1122. doi: 10.1161/CIRCULATIONAHA.122.058683. Epub 2022 Apr 11. Circulation. 2022. PMID: 35404677 No abstract available.
References
-
- The International Cardiac Collaborative on Neurodevelopment (ICCON) Investigators. Impact of operative and postoperative factors on neurodevelopmental outcomes after cardiac operations. Ann Thorac Surg. 2016;102:843–849. - PubMed
-
- Schaefer C, von Rhein M, Knirsch W, Huber R, Natalucci G, Caflisch J, Landolt MA and Latal B. Neurodevelopmental outcome, psychological adjustment, and quality of life in adolescents with congenital heart disease. Dev Med Child Neurol. 2013;55:1143–1149. - PubMed
-
- Newburger JW, Sleeper LA, Bellinger DC, Goldberg CS, Tabbutt S, Lu M, Mussatto KA, Williams IA, Gustafson KE, Mital S, et al. Early developmental outcome in children with hypoplastic left heart syndrome and related anomalies: the single ventricle reconstruction trial. Circulation. 2012;125:2081–2091. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
