

Physical and mental health 3 months after SARS-CoV-2 infection (long COVID) among adolescents in England (CLoCk): a national matched cohort study
- PMID: 35143770
- PMCID: PMC8820961
- DOI: 10.1016/S2352-4642(22)00022-0
Physical and mental health 3 months after SARS-CoV-2 infection (long COVID) among adolescents in England (CLoCk): a national matched cohort study
Erratum in
-
Correction to Lancet Child Adolesc Health 2022; 6: 230-39.Lancet Child Adolesc Health. 2022 Jul;6(7):e21. doi: 10.1016/S2352-4642(22)00151-1. Epub 2022 May 6. Lancet Child Adolesc Health. 2022. PMID: 35526538 Free PMC article. No abstract available.
Abstract
Background: We describe post-COVID symptomatology in a non-hospitalised, national sample of adolescents aged 11-17 years with PCR-confirmed SARS-CoV-2 infection compared with matched adolescents with negative PCR status.
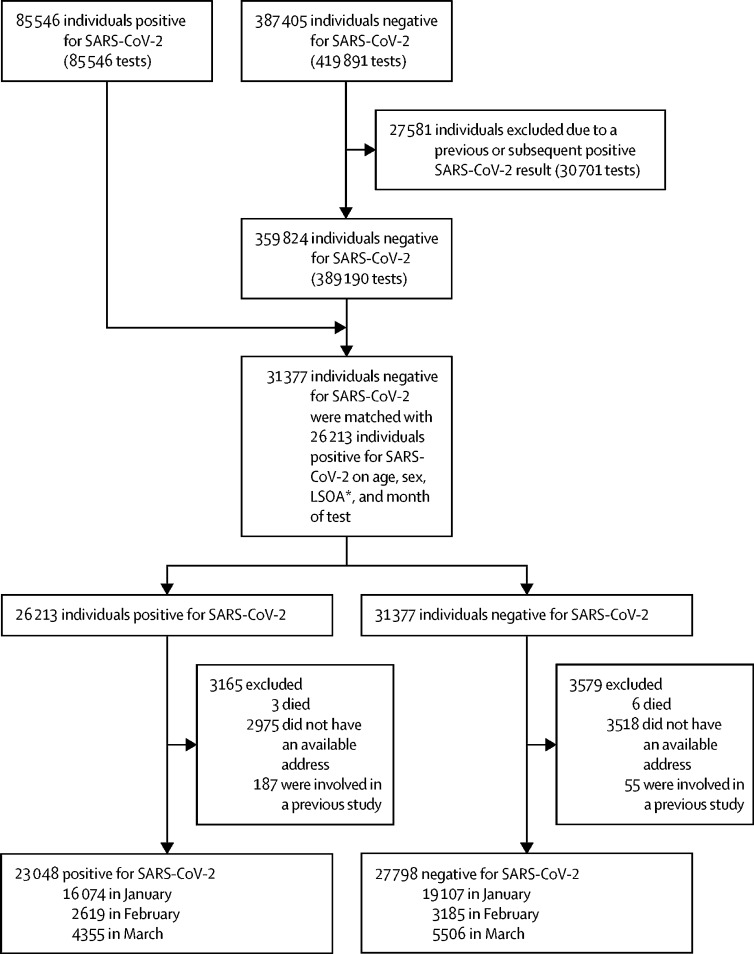
Methods: In this national cohort study, adolescents aged 11-17 years from the Public Health England database who tested positive for SARS-CoV-2 between January and March, 2021, were matched by month of test, age, sex, and geographical region to adolescents who tested negative. 3 months after testing, a subsample of adolescents were contacted to complete a detailed questionnaire, which collected data on demographics and their physical and mental health at the time of PCR testing (retrospectively) and at the time of completing the questionnaire (prospectively). We compared symptoms between the test-postive and test-negative groups, and used latent class analysis to assess whether and how physical symptoms at baseline and at 3 months clustered among participants. This study is registered with the ISRCTN registry (ISRCTN 34804192).
Findings: 23 048 adolescents who tested positive and 27 798 adolescents who tested negative between Jan 1, 2021, and March 31, 2021, were contacted, and 6804 adolescents (3065 who tested positive and 3739 who tested negative) completed the questionnaire (response rate 13·4%). At PCR testing, 1084 (35·4%) who tested positive and 309 (8·3%) who tested negative were symptomatic and 936 (30·5%) from the test-positive group and 231 (6·2%) from the test-negative group had three or more symptoms. 3 months after testing, 2038 (66·5%) who tested positive and 1993 (53·3%) who tested negative had any symptoms, and 928 (30·3%) from the test-positive group and 603 (16·2%) from the test-negative group had three or more symptoms. At 3 months after testing, the most common symptoms among the test-positive group were tiredness (1196 [39·0%]), headache (710 [23·2%]), and shortness of breath (717 [23·4%]), and among the test-negative group were tiredness (911 [24·4%]), headache (530 [14·2%]), and other (unspecified; 590 [15·8%]). Latent class analysis identified two classes, characterised by few or multiple symptoms. The estimated probability of being in the multiple symptom class was 29·6% (95% CI 27·4-31·7) for the test-positive group and 19·3% (17·7-21·0) for the test-negative group (risk ratio 1·53; 95% CI 1·35-1·70). The multiple symptoms class was more frequent among those with positive PCR results than negative results, in girls than boys, in adolescents aged 15-17 years than those aged 11-14 years, and in those with lower pretest physical and mental health.
Interpretation: Adolescents who tested positive for SARS-CoV-2 had similar symptoms to those who tested negative, but had a higher prevalence of single and, particularly, multiple symptoms at the time of PCR testing and 3 months later. Clinicians should consider multiple symptoms that affect functioning and recognise different clusters of symptoms. The multiple and varied symptoms show that a multicomponent intervention will be required, and that mental and physical health symptoms occur concurrently, reflecting their close relationship.
Funding: UK Department of Health and Social Care, in their capacity as the National Institute for Health Research, and UK Research and Innovation.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests TS is Chair of the Health Research Authority and therefore recused himself from the research ethics application. TC is a member of the National Institute for Health and Care Excellence committee for long COVID. She has written self-help books on chronic fatigue and has done workshops on chronic fatigue and post infectious syndromes. All other authors declare no competing interests.
Figures
Comment in
-
Assessing the impact of the pandemic in children and adolescents: SARS-CoV-2 infection and beyond.Lancet Child Adolesc Health. 2022 Apr;6(4):216-217. doi: 10.1016/S2352-4642(22)00035-9. Epub 2022 Feb 8. Lancet Child Adolesc Health. 2022. PMID: 35143769 Free PMC article. No abstract available.
References
-
- Chevinsky JR, Tao G, Lavery AM, et al. Late conditions diagnosed 1-4 months following an initial coronavirus disease 2019 (COVID-19) encounter: a matched-cohort study using inpatient and outpatient administrative data—United States, March 1–June 30, 2020. Clin Infect Dis. 2021;73(suppl 1):S5–16. - PMC - PubMed
-
- Spiegelhalter D, Masters A. Penguin Random House; UK: 2021. Covid by numbers: making sense of the pandemic with data.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
