

Diabetes mortality and trends before 25 years of age: an analysis of the Global Burden of Disease Study 2019
- PMID: 35143780
- PMCID: PMC8860753
- DOI: 10.1016/S2213-8587(21)00349-1
Diabetes mortality and trends before 25 years of age: an analysis of the Global Burden of Disease Study 2019
Abstract
Background: Diabetes, particularly type 1 diabetes, at younger ages can be a largely preventable cause of death with the correct health care and services. We aimed to evaluate diabetes mortality and trends at ages younger than 25 years globally using data from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019.
Methods: We used estimates of GBD 2019 to calculate international diabetes mortality at ages younger than 25 years in 1990 and 2019. Data sources for causes of death were obtained from vital registration systems, verbal autopsies, and other surveillance systems for 1990-2019. We estimated death rates for each location using the GBD Cause of Death Ensemble model. We analysed the association of age-standardised death rates per 100 000 population with the Socio-demographic Index (SDI) and a measure of universal health coverage (UHC) and described the variability within SDI quintiles. We present estimates with their 95% uncertainty intervals.
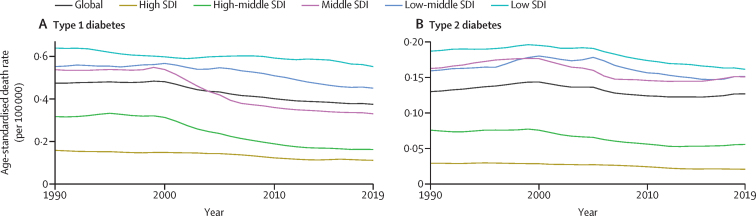
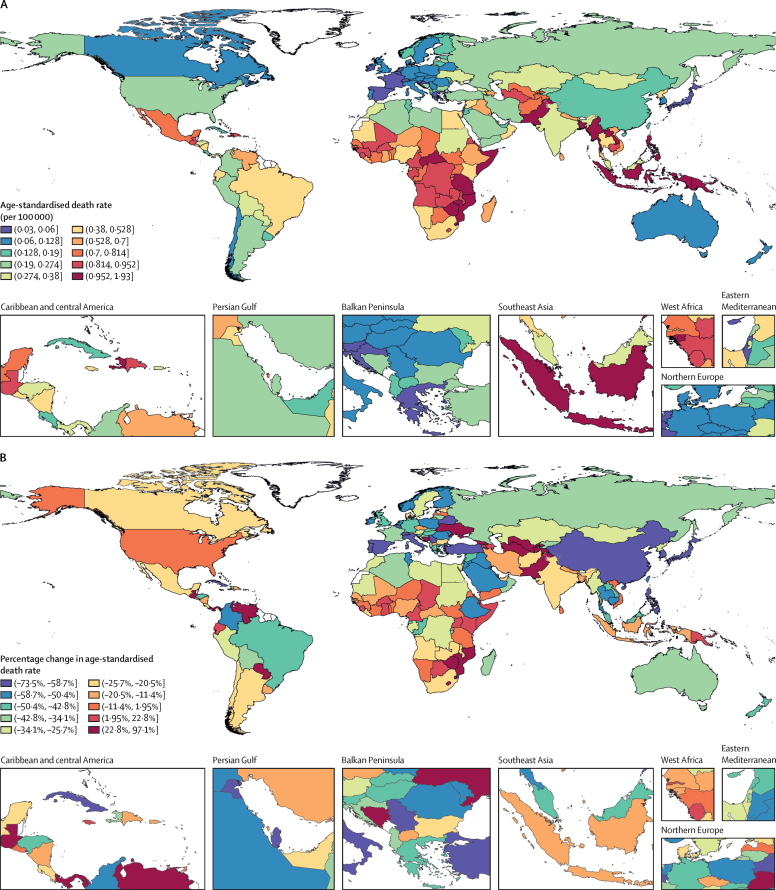
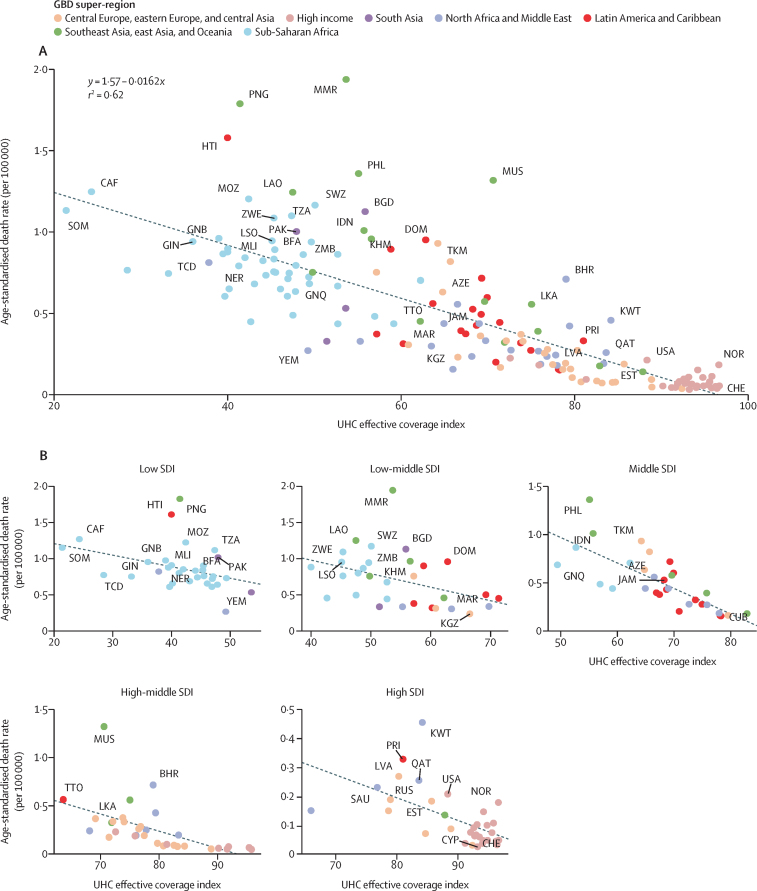
Findings: In 2019, 16 300 (95% uncertainty interval 14 200 to 18 900) global deaths due to diabetes (type 1 and 2 combined) occurred in people younger than 25 years and 73·7% (68·3 to 77·4) were classified as due to type 1 diabetes. The age-standardised death rate was 0·50 (0·44 to 0·58) per 100 000 population, and 15 900 (97·5%) of these deaths occurred in low to high-middle SDI countries. The rate was 0·13 (0·12 to 0·14) per 100 000 population in the high SDI quintile, 0·60 (0·51 to 0·70) per 100 000 population in the low-middle SDI quintile, and 0·71 (0·60 to 0·86) per 100 000 population in the low SDI quintile. Within SDI quintiles, we observed large variability in rates across countries, in part explained by the extent of UHC (r2=0·62). From 1990 to 2019, age-standardised death rates decreased globally by 17·0% (-28·4 to -2·9) for all diabetes, and by 21·0% (-33·0 to -5·9) when considering only type 1 diabetes. However, the low SDI quintile had the lowest decline for both all diabetes (-13·6% [-28·4 to 3·4]) and for type 1 diabetes (-13·6% [-29·3 to 8·9]).
Interpretation: Decreasing diabetes mortality at ages younger than 25 years remains an important challenge, especially in low and low-middle SDI countries. Inadequate diagnosis and treatment of diabetes is likely to be major contributor to these early deaths, highlighting the urgent need to provide better access to insulin and basic diabetes education and care. This mortality metric, derived from readily available and frequently updated GBD data, can help to monitor preventable diabetes-related deaths over time globally, aligned with the UN's Sustainable Development Targets, and serve as an indicator of the adequacy of basic diabetes care for type 1 and type 2 diabetes across nations.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests J L Baker reports non-financial support as an unpaid speaker at Novo Nordisk symposiums (outside the submitted work). S Bhaskar reports institutional support from NSW Health Pathology (Australia), grants or contracts from the New South Wales (NSW) Ministry of Health NSW Brain Clot Bank (2019–22) in Australia, and paid or unpaid leadership or fiduciary roles in board, society, committee, or advocacy groups with the Rotary Club of Sydney (NSW, Australia) as a board director and chair of the Youth Committee and with the International Rotary Fellowship of Healthcare Professionals as board director (all outside the submitted work). I Y Elgendy acknowledges grants from Caladrius Biosciences, outside the submitted work. D Flood reports grants or contracts from US National Institutes of Health (NIH) funding comparative health systems research on diabetes indicators (grant P30-DK09292); unpaid leadership or fiduciary roles in board, society, committee, or advocacy groups with Maya Health Alliance as lead diabetes physician for this non-governmental clinical organisation in Guatemala, conducting unpaid advocacy on behalf of people with diabetes; and stock or stock options as co-founder and 1% co-owner of GlucoSalud, a diabetes social business in Guatemala (all outside the submitted work). N Ghith reports support for the present manuscript via a grant from the Novo Nordisk Foundation (NNF16OC0021856). N E Ismail reports an unpaid leadership or fiduciary role in board, society, committee, or advocacy group, with the Malaysian Academy of Pharmacy as a council member (outside the submitted work). K Krishan reports non-financial support from the UGC Centre of Advanced Study, CAS II, Department of Anthropology, Panjab University, Chandigarh, India (outside the submitted work). U O Mueller reports a grant from the US National Institute of Aging to the University of Washington, granted as a subaward to the Center for Population and Health, and paid or unpaid leadership or fiduciary roles in board, society, committee, or advocacy group with the Center for Population and Health as the chairman (all outside the submitted work). M P Schlaich reports grants or contracts from Boehringer Ingelheim in support for an investigator-initiated study with SGLT-2 inhibitors in patients with diabetes (outside the submitted work). J A Singh reports consulting fees from Crealta/Horizon, Medisys, Fidia, PK Med, Two Labs, Adept Field Solutions, Clinical Care Options, Clearview Healthcare Partners, Putnam Associates, FocusForward, Navigant Consulting, Spherix, MedIQ, Jupiter Life Science, UBM, Trio Health, Medscape, WebMD, Practice Point communications, the NIH, and the American College of Rheumatology; payment or honoraria for lectures, presentations, speakers' bureaus, manuscript writing, or educational events from Simply Speaking; support for attending meetings or travel from OMERACT, an international organisation that develops measures for clinical trials and receives arm's length funding from 12 pharmaceutical companies, when travelling to OMERACT meetings; participation on a data safety monitoring board or an advisory board as a member of the US Food and Drug Administration Arthritis Advisory Committee; paid or unpaid leadership or fiduciary roles in board, society, committee, or advocacy groups with OMERACT as a member of the steering committee, with the Veterans Affairs Rheumatology Field Advisory Committee as a chair member, and with the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis as director and editor; stock or stock options in TPT Global Tech, Vaxart Pharmaceuticals, Atyu Biopharma, and Charlotte's Web Holdings and previously owned stock options in Amarin, Viking, and Moderna pharmaceuticals (all outside the submitted work). M Tonelli reports payment or honoraria for lectures, presentations, speakers' bureaus, manuscript writing, or educational events from AstraZeneca (outside the submitted work). R Uddin reports grants from Deakin University (Geelong, VIC, Australia) through an Alfred Deakin Postdoctoral Research Fellowship and support for attending meetings or travel from the Deakin University Institute for Physical Activity and Nutrition (all outside the submitted work). S Zadey reports unpaid leadership or fiduciary roles in other board, society, committee, or advocacy groups with the Association for Socially Applicable Research as the co-founding director.
Figures
Comment in
-
Prevention of diabetes mortality at ages younger than 25 years: access to medications and high-quality health care.Lancet Diabetes Endocrinol. 2022 Mar;10(3):151-152. doi: 10.1016/S2213-8587(22)00009-2. Epub 2022 Feb 7. Lancet Diabetes Endocrinol. 2022. PMID: 35143781 No abstract available.
References
-
- WHO Global action plan for the prevention and control of noncommunicable diseases: 2013-2020. 2013. http://apps.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf
-
- UN Transforming our world: the 2030 agenda for sustainable development. 2015. https://sdgs.un.org/2030agenda
-
- Vanelli M, Chiari G, Ghizzoni L, Costi G, Giacalone T, Chiarelli F. Effectiveness of a prevention program for diabetic ketoacidosis in children. An 8-year study in schools and private practices. Diabetes Care. 1999;22:7–9. - PubMed
