

Nomogram to predict rapid kidney function decline in population at risk of cardiovascular disease
- PMID: 35144580
- PMCID: PMC8830119
- DOI: 10.1186/s12882-022-02696-9
Nomogram to predict rapid kidney function decline in population at risk of cardiovascular disease
Abstract
Background: To develop a reliable model to predict rapid kidney function decline (RKFD) among population at risk of cardiovascular disease.
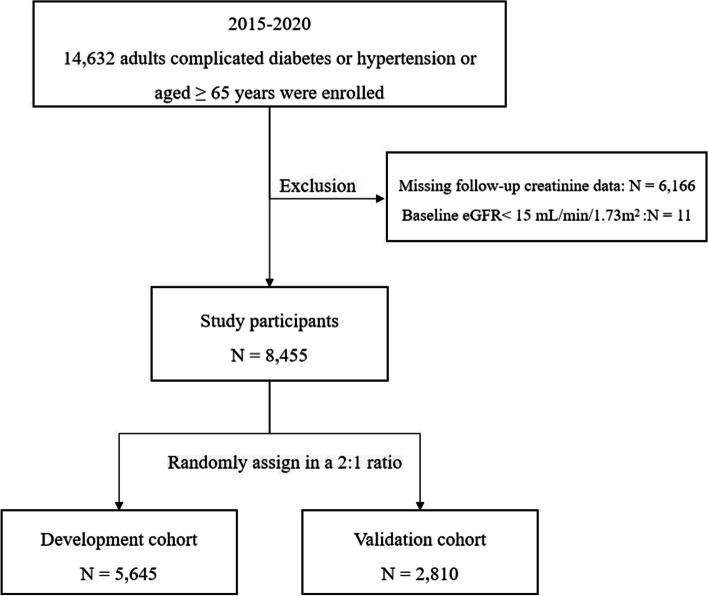
Methods: In this retrospective study, key monitoring residents including the elderly, and patients with hypertension or diabetes of China National Basic Public Health Service who underwent community annual physical examinations from January 2015 to December 2020 were included. Healthy records were extracted from regional chronic disease management platform. RKFD was defined as the reduction of estimated glomerular filtration rate (eGFR) ≥ 40% during follow-up period. The entire cohort were randomly assigned to a development cohort and a validation cohort in a 2:1 ratio. Cox regression analysis was used to identify the independent predictors. A nomogram was established based on the development cohort. The concordance index (C-index) and calibration plots were calculated. Decision curve analysis was applied to evaluate the clinical utility.
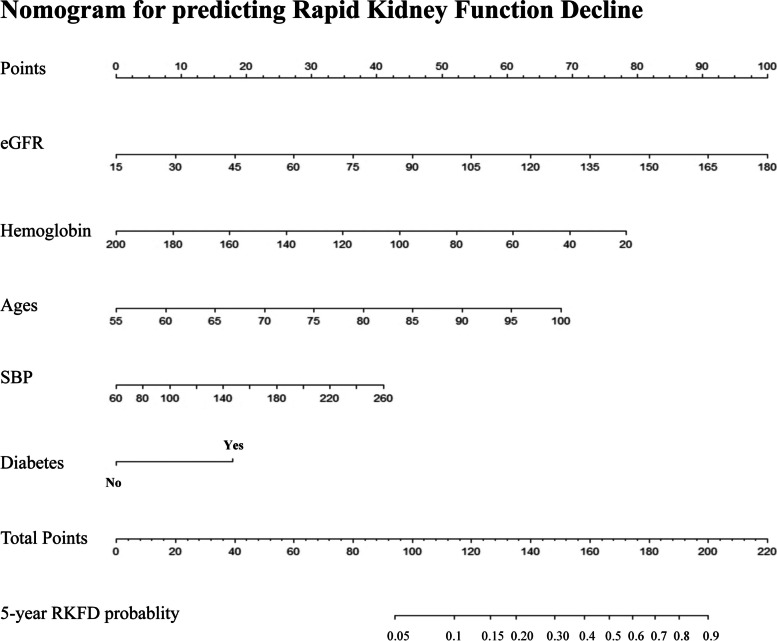
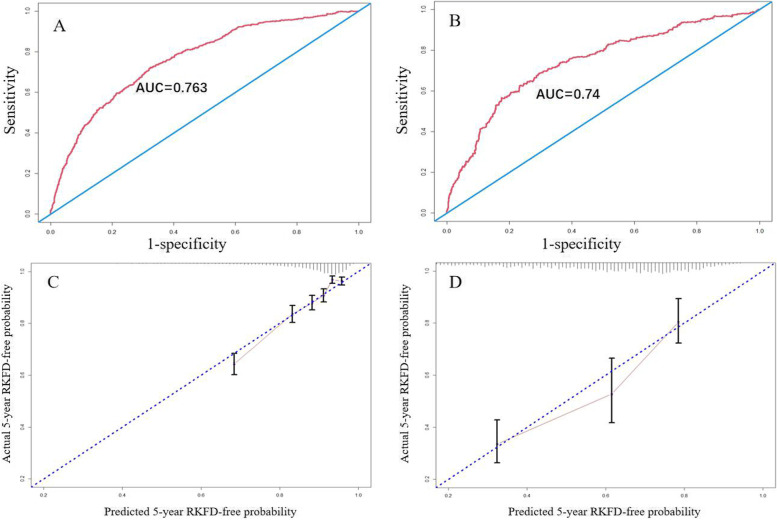
Results: A total of 8455 subjects were included. During the median follow-up period of 3.72 years, the incidence of RKFD was 11.96% (n = 1011), 11.98% (n = 676) and 11.92% (n = 335) in the entire cohort, development cohort and validation cohort, respectively. Age, eGFR, hemoglobin, systolic blood pressure, and diabetes were identified as predictors for RKFD. Good discriminating performance was observed in both the development (C-index, 0.73) and the validation (C-index, 0.71) cohorts, and the AUCs for predicting 5-years RKFD was 0.763 and 0.740 in the development and the validation cohort, respectively. Decision curve analysis further confirmed the clinical utility of the nomogram.
Conclusions: Our nomogram based on five readily accessible variables (age, eGFR, hemoglobin, systolic blood pressure, and diabetes) is a useful tool to identify high risk patients for RKFD among population at risk of cardiovascular disease in primary care. Whereas, further external validations are needed before clinical generalization.
Keywords: Cardiovascular disease; Rapid kidney function decline; Risk prediction model.
© 2022. The Author(s).
Conflict of interest statement
None of authors declared potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Collaborator GDAI. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392:1785–1789. doi: 10.1016/S0140-6736(18)32279-7. - DOI - PMC - PubMed
-
- Malhotra R, Katz R, Jotwani V, Agarwal A, Cohen DL, Cushman WC, et al. Estimated GFR variability and risk of cardiovascular events and mortality in SPRINT (systolic blood pressure intervention trial). American journal of kidney diseases : the official journal of the National Kidney Foundation. 2020. 10.1053/j.ajkd.2020.10.016. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
