

Immune Checkpoint Therapies and Atherosclerosis: Mechanisms and Clinical Implications: JACC State-of-the-Art Review
- PMID: 35144750
- PMCID: PMC8983019
- DOI: 10.1016/j.jacc.2021.11.048
Immune Checkpoint Therapies and Atherosclerosis: Mechanisms and Clinical Implications: JACC State-of-the-Art Review
Abstract
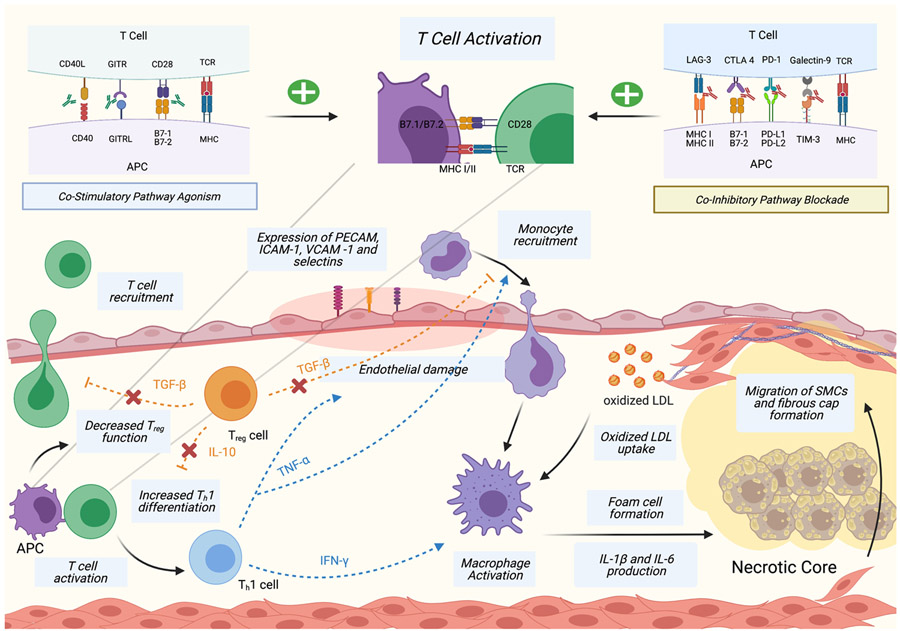
Immune checkpoint inhibitor therapy has revolutionized the treatment of advanced malignancies in recent years. Numerous reports have detailed the myriad of possible adverse inflammatory effects of immune checkpoint therapies, including within the cardiovascular system. However, these reports have been largely limited to myocarditis. The critical role of inflammation and adaptive immunity in atherosclerosis has been well characterized in preclinical studies, and several emerging clinical studies indicate a potential role of immune checkpoint targeting therapies in the development and exacerbation of atherosclerosis. In this review, we provide an overview of the role of T-cell immunity in atherogenesis and describe the molecular effects and clinical associations of both approved and investigational immune checkpoint therapy on atherosclerosis. We also highlight the role of cholesterol metabolism in oncogenesis and discuss the implications of these associations on future treatment and monitoring of atherosclerotic cardiovascular disease in the oncologic population receiving immune checkpoint therapy.
Keywords: atherosclerosis; cardio-oncology; cardiovascular disease; immunology; inflammation.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Drs Stein-Merlob and Nayeri are supported by the National Institutes of Health Cardiovascular Scientist Training Program (grant T32HL007895). Dr Sallam is supported by the American Heart Association Transformational Project Award and the National Institutes of Health grant HL149766. Dr Neilan is supported by a gift from A. Curt Greer and Pamela Kohlberg, and grants from the National Institutes of Health/National Heart, Lung, and Blood Institute grants R01HL130539, R01HL137562, and K24HL150238. Dr Yang is supported by a grant from CSL Behring. Dr Neilan has been a consultant to and received fees from Amgen, H3-Biomedicine, and AbbVie outside of the current work; has received consultant fees from Bristol Myers Squibb for a Scientific Advisory Board focused on myocarditis related to immune checkpoint inhibitors; and has received grant funding from AstraZeneca on atherosclerosis with immune checkpoint inhibitors. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


References
-
- Dunn GP, Bruce AT, Ikeda H, Old LJ, Shreiber RD. Cancer Immunoediting: From Surveillance to Escape. Cancer Immunother. Immune Suppr. Tumor Growth Second Ed. 2013;3:85–99.
-
- Balar AV, Castellano D, O’Donnell PH, et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): a multicentre, single-arm, phase 2 study. Lancet Oncol. 2017;18:1483–1492. Available at: 10.1016/S1470-2045(17)30616-2. - DOI - PubMed
