

Clinical predictors of acute cardiac injury and normalization of troponin after hospital discharge from COVID-19
- PMID: 35144887
- PMCID: PMC8819639
- DOI: 10.1016/j.ebiom.2022.103821
Clinical predictors of acute cardiac injury and normalization of troponin after hospital discharge from COVID-19
Abstract
Background: Although acute cardiac injury (ACI) is a known COVID-19 complication, whether ACI acquired during COVID-19 recovers is unknown. This study investigated the incidence of persistent ACI and identified clinical predictors of ACI recovery in hospitalized patients with COVID-19 2.5 months post-discharge.
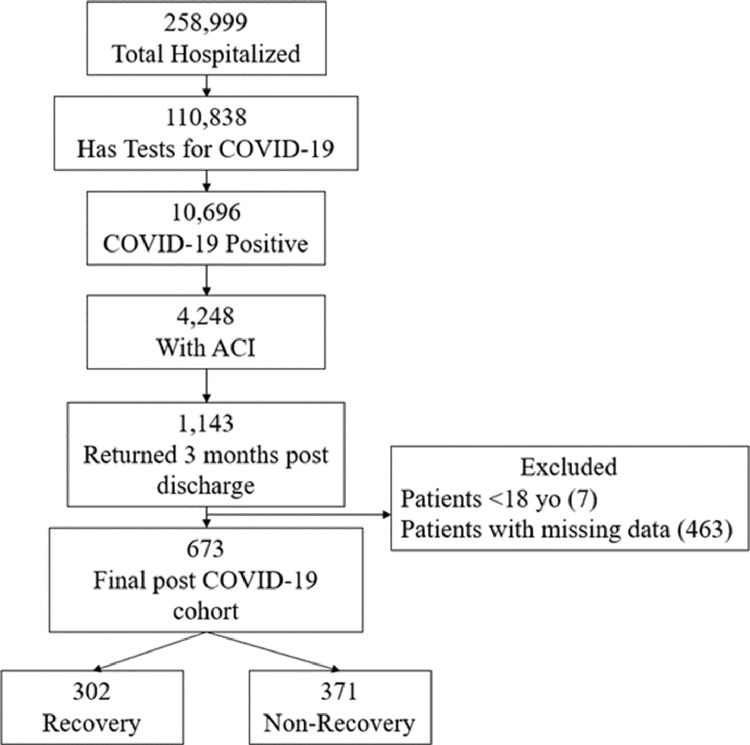
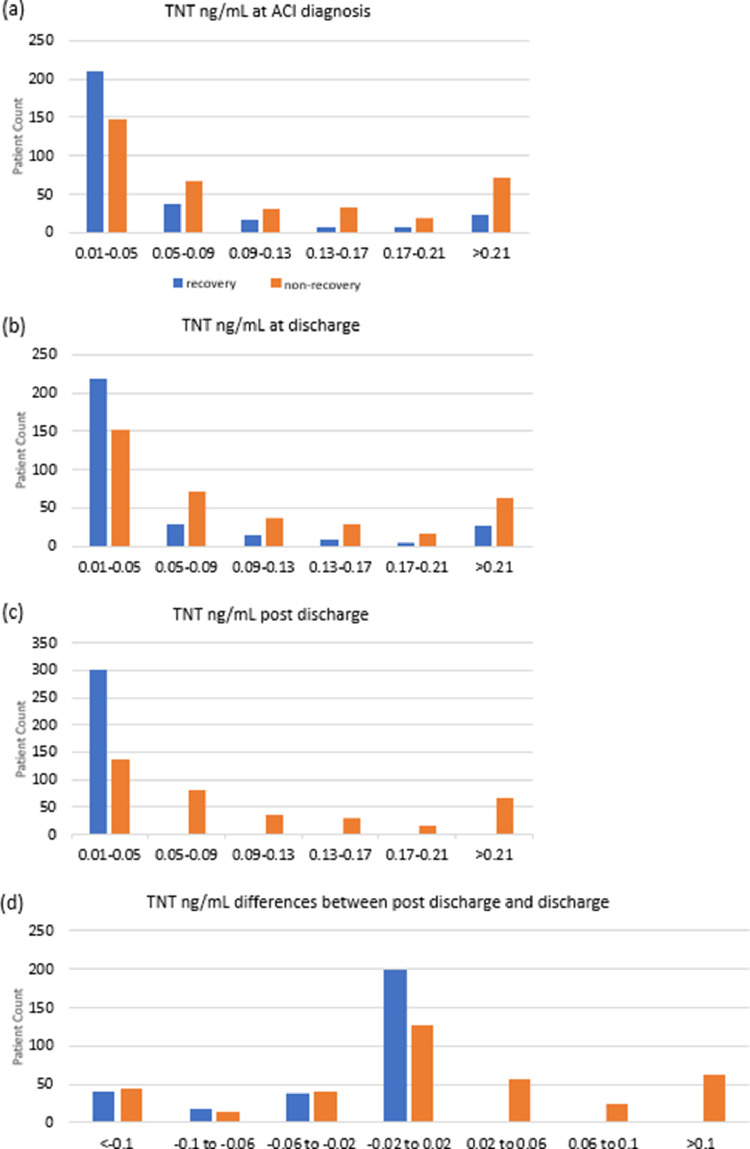
Methods: This retrospective study consisted of 10,696 hospitalized COVID-19 patients from March 11, 2020 to June 3, 2021. Demographics, comorbidities, and laboratory tests were collected at ACI onset, hospital discharge, and 2.5 months post-discharge. ACI was defined as serum troponin-T (TNT) level >99th-percentile upper reference limit (0.014ng/mL) during hospitalization, and recovery was defined as TNT below this threshold 2.5 months post-discharge. Four models were used to predict ACI recovery status.
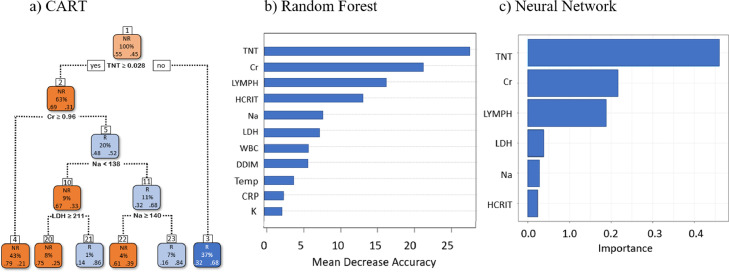
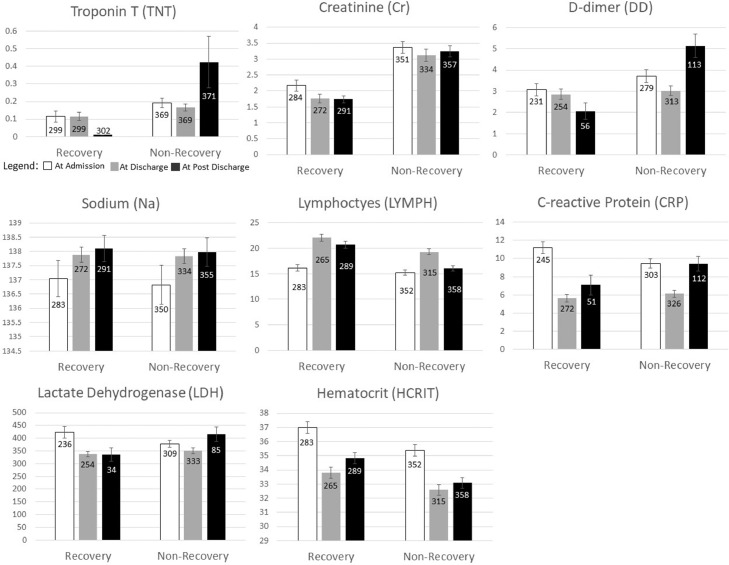
Results: There were 4,248 (39.7%) COVID-19 patients with ACI, with most (93%) developed ACI on or within a day after admission. In-hospital mortality odds ratio of ACI patients was 4.45 [95%CI: 3.92, 5.05, p<0.001] compared to non-ACI patients. Of the 2,880 ACI survivors, 1,114 (38.7%) returned to our hospitals 2.5 months on average post-discharge, of which only 302 (44.9%) out of 673 patients recovered from ACI. There were no significant differences in demographics, race, ethnicity, major commodities, and length of hospital stay between groups. Prediction of ACI recovery post-discharge using the top predictors (troponin, creatinine, lymphocyte, sodium, lactate dehydrogenase, lymphocytes and hematocrit) at discharge yielded 63.73%-75.73% accuracy.
Interpretation: Persistent cardiac injury is common among COVID-19 survivors. Readily available patient data accurately predict ACI recovery post-discharge. Early identification of at-risk patients could help prevent long-term cardiovascular complications.
Funding: None.
Keywords: Machine learning; SARS-CoV-2; acute myocardial injury; heart failure.
Copyright © 2022 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declared no competing interests.
Figures
Comment in
-
Persistent cardiac injury - An important component of long COVID-19 syndrome.EBioMedicine. 2022 Mar;77:103892. doi: 10.1016/j.ebiom.2022.103892. Epub 2022 Feb 23. EBioMedicine. 2022. PMID: 35219086 Free PMC article. No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
