

Updated Integrated Analysis of the Efficacy and Safety of Entrectinib in Patients With NTRK Fusion-Positive Solid Tumors
- PMID: 35144967
- PMCID: PMC9365368
- DOI: 10.1158/1078-0432.CCR-21-3597
Updated Integrated Analysis of the Efficacy and Safety of Entrectinib in Patients With NTRK Fusion-Positive Solid Tumors
Erratum in
-
Correction: Updated Integrated Analysis of the Efficacy and Safety of Entrectinib in Patients with NTRK Fusion-Positive Solid Tumors.Clin Cancer Res. 2022 May 13;28(10):2196. doi: 10.1158/1078-0432.CCR-22-1108. Clin Cancer Res. 2022. PMID: 35553647 Free PMC article. No abstract available.
Abstract
Purpose: Entrectinib potently inhibits tropomyosin receptor kinases (TRKAs)/B/C and ROS1, and previously induced deep [objective response rate (ORR) 57.4%] and durable [median duration of response (DoR) 10.4 months] responses in adults with NTRK fusion-positive solid tumors from three phase I/II trials. This article expands prior reports with additional patients and longer follow-up.
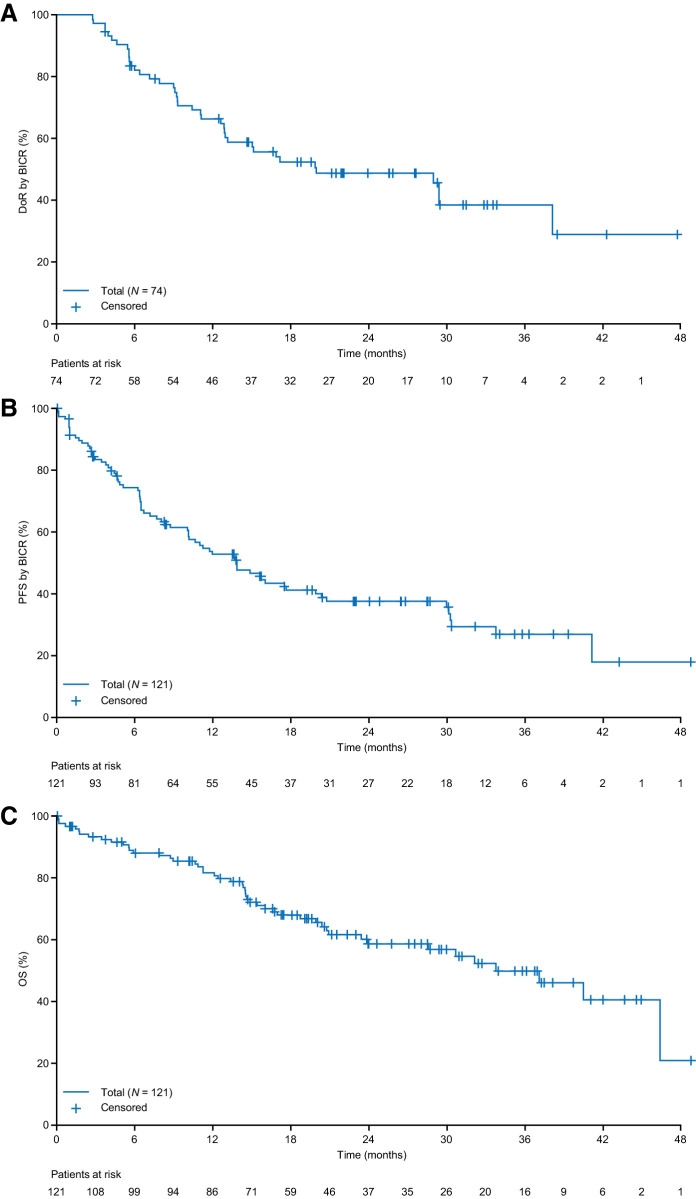
Patients and methods: Patients with locally advanced/metastatic NTRK fusion-positive solid tumors and ≥12 months' follow-up were included. Primary endpoints were ORR and DoR by blinded independent central review (BICR); secondary endpoints included progression-free survival (PFS), intracranial efficacy, and safety. The safety-evaluable populations included all patients who had received ≥1 entrectinib dose.
Results: At clinical cut-off (August 31, 2020), the efficacy-evaluable population comprised 121 adults with 14 tumor types and ≥30 histologies. Median follow-up was 25.8 months; 61.2% of patients had a complete (n = 19) or partial response (n = 55). Median DoR was 20.0 months [95% confidence interval (CI), 13.0-38.2]; median PFS was 13.8 months (95% CI, 10.1-19.9). In 11 patients with BICR-assessed measurable central nervous system (CNS) disease, intracranial ORR was 63.6% (95% CI, 30.8-89.1) and median intracranial DoR was 22.1 (95% CI, 7.4-not estimable) months. The safety profile of entrectinib in adults and pediatric patients was aligned with previous reports. Most treatment-related adverse events (TRAEs) were grade 1/2 and manageable/reversible with dose modifications. TRAE-related discontinuations occurred in 8.3% of patients.
Conclusions: With additional clinical experience, entrectinib continues to demonstrate durable systemic and intracranial responses and can address the unmet need of a CNS-active treatment in patients with NTRK fusion-positive solid tumors.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
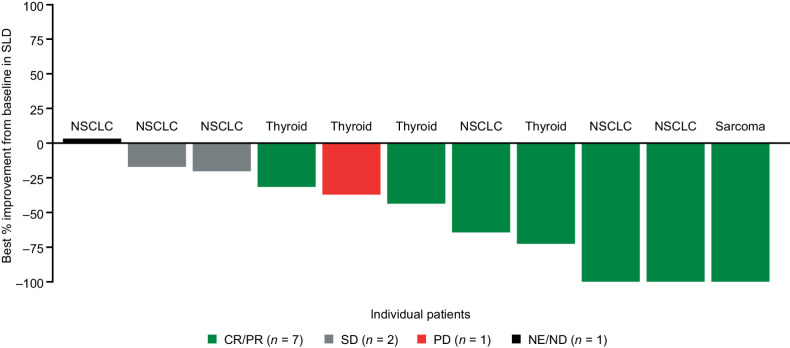
![Figure 1. Responses and time on entrectinib treatment in patients with NTRK fusion-positive solid tumors, by tumor type (BICR assessed). A, Best individual patient responses [n = 103; 18 patients with missing sum of the longest diameter (SLD) change were excluded from the plot]. B, Time on entrectinib treatment. Data cut-off August 31, 2020. The minimum shrinkage in the SLD of target lesions that defined an OR was 30%. Gastrointestinal (GI)-other, adenocarcinoma of upper GI tract; CRC, colorectal carcinoma; CUP, cancer of unknown primary; Inv, investigator; ND, not determined; SD, stable disease.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/75dd/9365368/39f0f639579d/1302fig1.jpg)
References
-
- Rolfo C. NTRK gene fusions: a rough diamond ready to sparkle. Lancet Oncol 2020;21:472–4. - PubMed
