

A non-invasive method for concurrent detection of early-stage women-specific cancers
- PMID: 35145183
- PMCID: PMC8831619
- DOI: 10.1038/s41598-022-06274-9
A non-invasive method for concurrent detection of early-stage women-specific cancers
Abstract
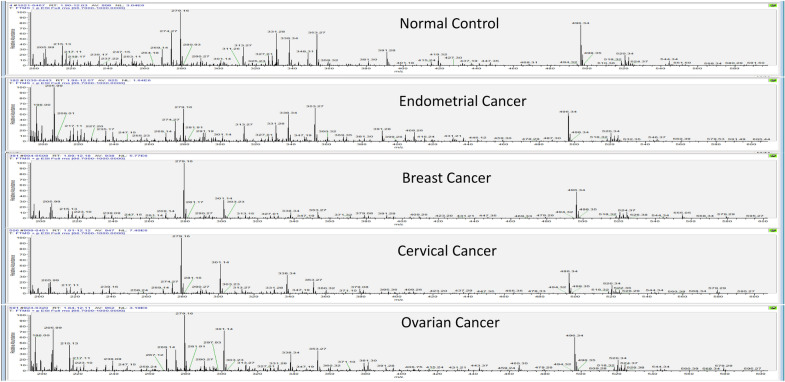
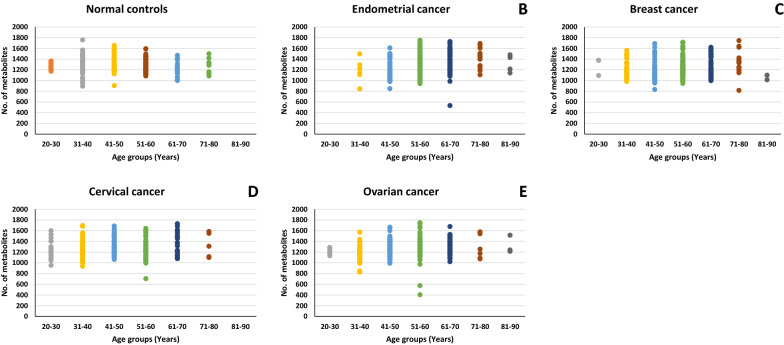
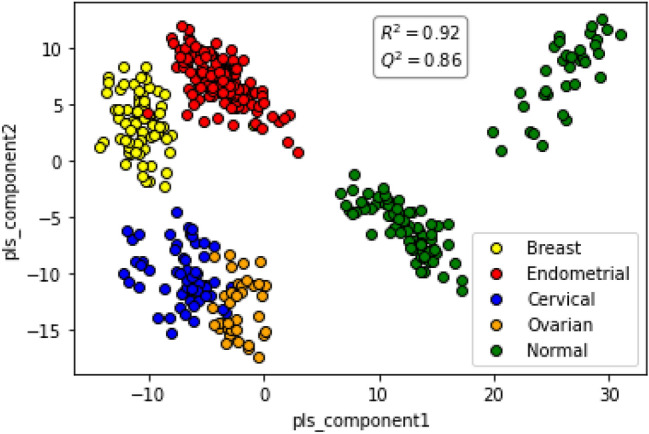
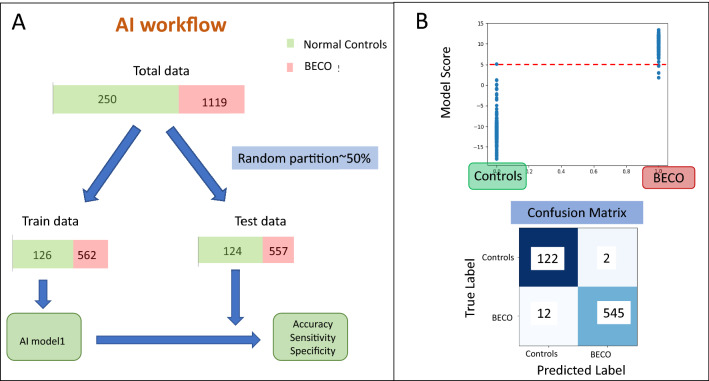
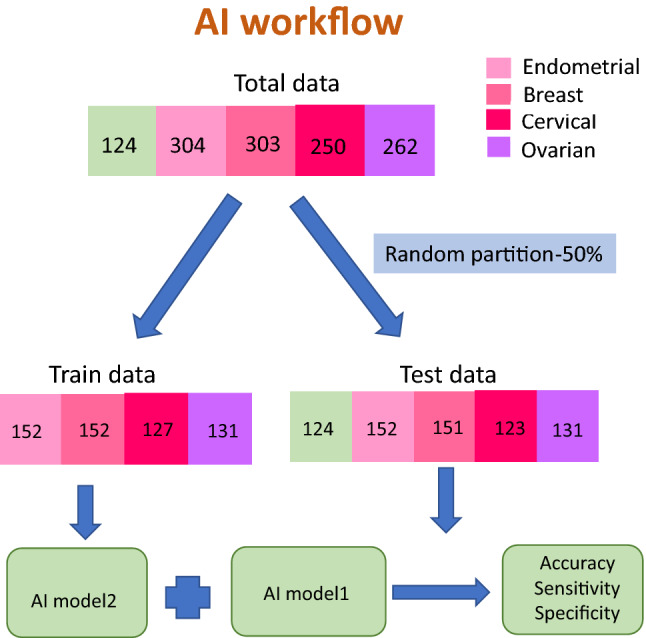
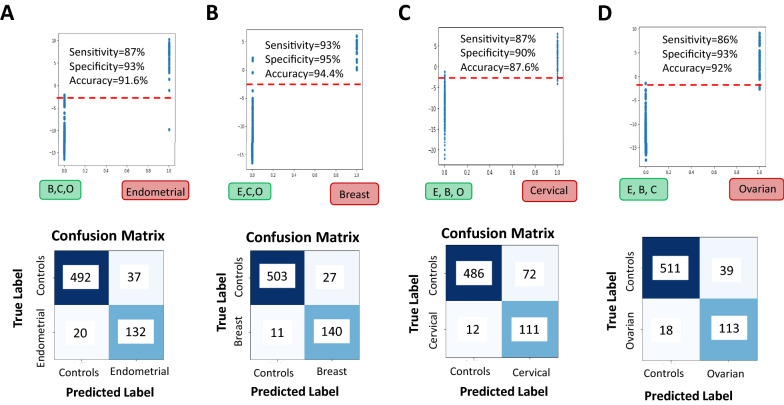
We integrated untargeted serum metabolomics using high-resolution mass spectrometry with data analysis using machine learning algorithms to accurately detect early stages of the women specific cancers of breast, endometrium, cervix, and ovary across diverse age-groups and ethnicities. A two-step approach was employed wherein cancer-positive samples were first identified as a group. A second multi-class algorithm then helped to distinguish between the individual cancers of the group. The approach yielded high detection sensitivity and specificity, highlighting its utility for the development of multi-cancer detection tests especially for early-stage cancers.
© 2022. The Author(s).
Conflict of interest statement
A.G, G.S., Z.S. and N.S. are fulltime employees of PredOmix Technologies Private Limited. K.V.S.R., R.A. and S.N. are cofounders and own stock in both PredOmix Technologies Private Limited and PredOmix, Inc. The work described in this report is the subject of an International PCT filing. Application No. PCT/US21/48337.
Figures

References
-
- Fitzmaurice C, Akinyemiju TF, Al Lami FH, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: A systematic analysis for the Global Burden of Disease study. JAMA Oncol. 2018;4:1553–1568. doi: 10.1001/jamaoncol.2018.2706. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
