

Risk factors, time to onset and recurrence of delirium in a mixed medical-surgical ICU population: A secondary analysis using Cox and CHAID decision tree modeling
- PMID: 35145366
- PMCID: PMC8822304
- DOI: 10.17179/excli2021-4381
Risk factors, time to onset and recurrence of delirium in a mixed medical-surgical ICU population: A secondary analysis using Cox and CHAID decision tree modeling
Abstract
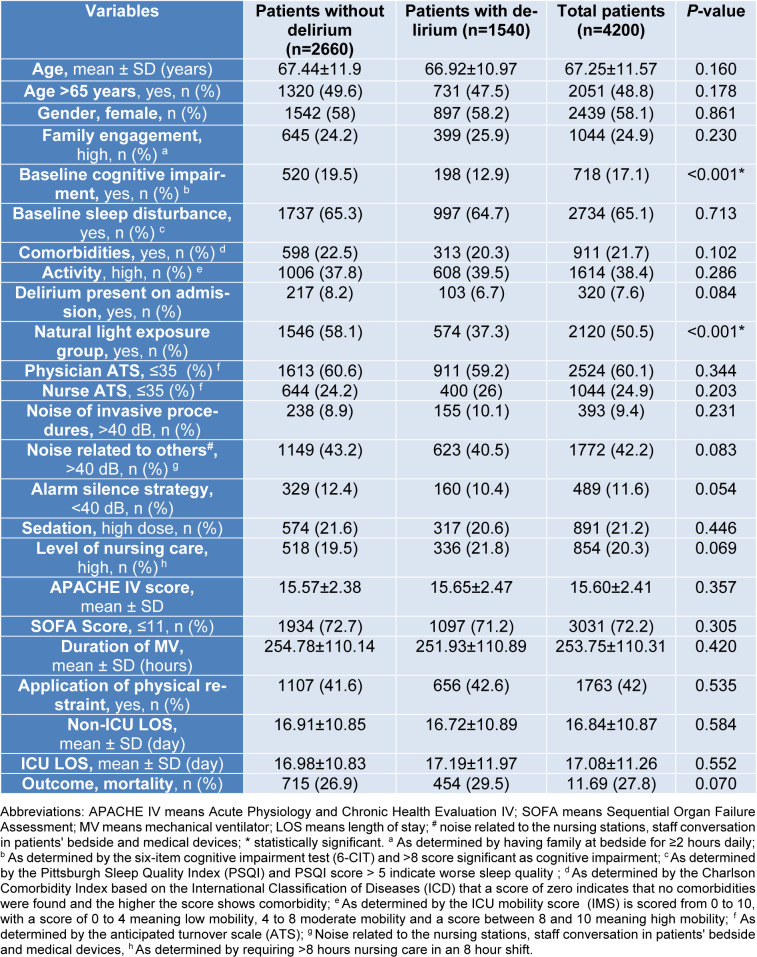
A retrospective secondary analysis of 4,200 patients was collected from two academic medical centers. Delirium was assessed using the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) in all patients. Univariate and multivariate Cox models, logistic regression analysis, and Chi-square Automatic Interaction Detector (CHAID) decision tree modeling were used to explore delirium risk factors. Increased delirium risk was associated with exposed only to artificial light (AL) hazard ratio (HR) 1.84 (95 % CI: 1.66-2.044, P<0.001), physical restraint application 1.11 (95 % CI: 1.001-1.226, P=0.049), and high nursing care requirements (>8 hours per 8-hour shift) 1.18 (95 % CI: 1.048-1.338, P=0.007). Delirium incidence was inversely associated with greater family engagement 0.092 (95 % CI: 0.014-0.596, P=0.012), low staff burnout and anticipated turnover scores 0.093 (95 % CI: 0.014-0.600, P=0.013), non-ICU length-of-stay (LOS)<15 days 0.725 (95 % CI: 0.655-0.804, P<0.001), and ICU LOS ≤15 days 0.509 (95 % CI: 0.456-0.567, P<0.001). CHAID modeling indicated that AL exposure and age <65 years were associated with a high risk of delirium incidence, whereas SOFA score ≤11, APACHE IV score >15 and natural light (NL) exposure were associated with moderate risk, and female sex was associated with low risk. More rapid time to delirium onset correlated with baseline sleep disturbance (P=0.049), high nursing care requirements (P=0.019), and prolonged ICU and non-ICU hospital LOS (P<0.001). Delirium recurrence correlated with age >65 years (HR 2.198; 95 % CI: 1.101-4.388, P=0.026) and high nursing care requirements (HR 1.978, 95 % CI: 1.096-3.569), with CHAID modeling identifying AL exposure (P<0.001) and age >65 years (P=0.032) as predictive variables. Development of ICU delirium correlated with application of physical restraints, high nursing care requirements, prolonged ICU and non-ICU LOS, exposure exclusively to AL (rather than natural), less family engagement, and greater staff burnout and anticipated turnover scores. ICU delirium occurred more rapidly in patients with baseline sleep disturbance, and recurrence correlated with the presence of delirium on ICU admission, exclusive AL exposure, and high nursing care requirements.
Keywords: Intensive Care Units; Iran; critical care; delirium; risk factors.
Copyright © 2022 Rahimibashar et al.
Figures






References
-
- Adams A, Hollingsworth A, Osman A. The implementation of a cultural change toolkit to reduce nursing burnout and mitigate nurse turnover in the emergency department. J Emerg Nurs. 2019;45:452–456. - PubMed
-
- American Psychiatric Association. Diagnostic and statistical manual. 5th ed. Washington, DC: APA Press; 2013.
-
- Arenson BG, Macdonald LA, Grocott HP, Hiebert BM, Arora RC. Effect of intensive care unit environment on in-hospital delirium after cardiac surgery. J Thorac Cardiovasc Surg. 2013;146:172–178. - PubMed
-
- Barlow KM, Zangaro GA. Meta-analysis of the reliability and validity of the Anticipated Turnover Scale across studies of registered nurses in the United States. J Nurs Manag. 2010;18:862–873. - PubMed
LinkOut - more resources
Full Text Sources