

Prevalence and predictors of adequate treatment of overt hypothyroidism - a population-based study
- PMID: 35145368
- PMCID: PMC8822305
- DOI: 10.17179/excli2021-4291
Prevalence and predictors of adequate treatment of overt hypothyroidism - a population-based study
Abstract
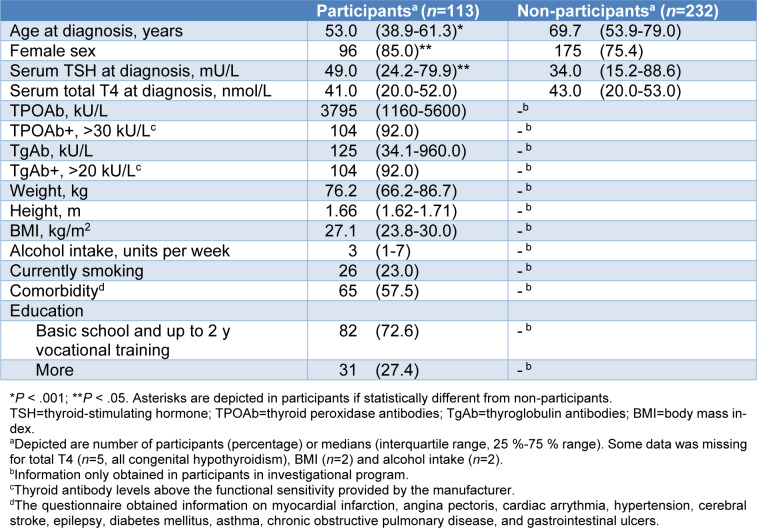
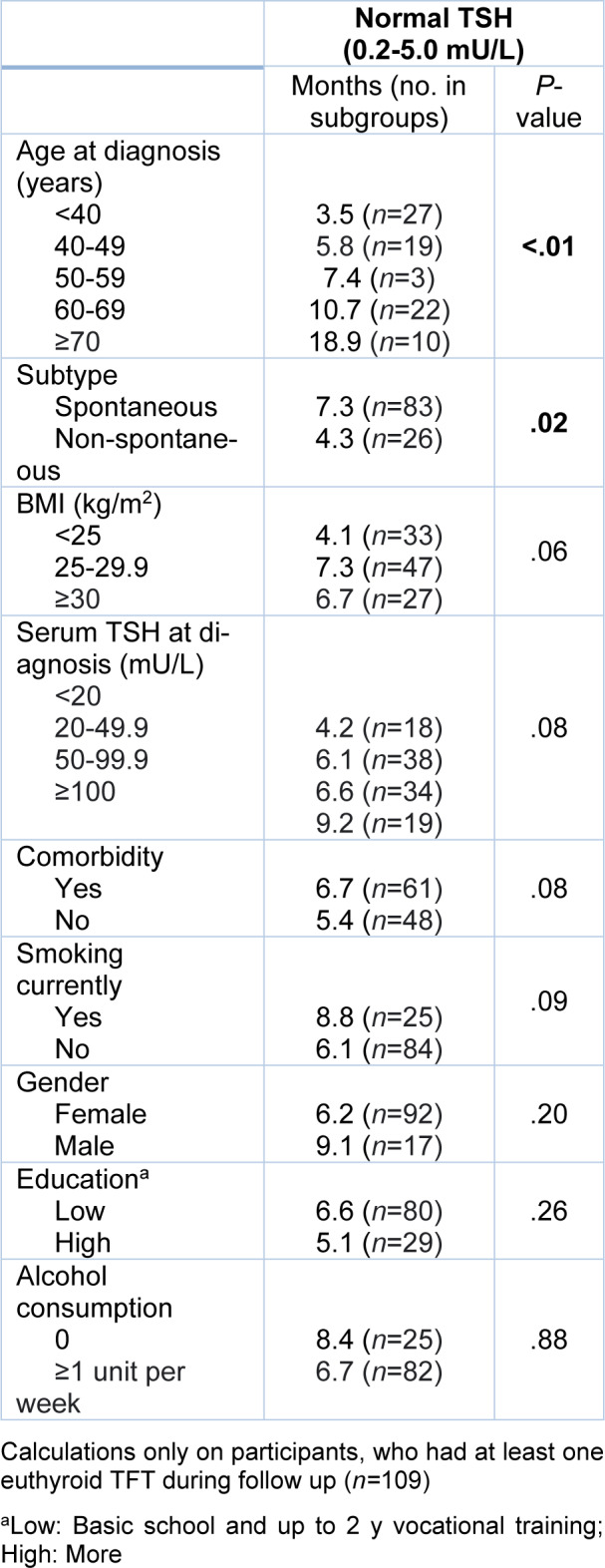
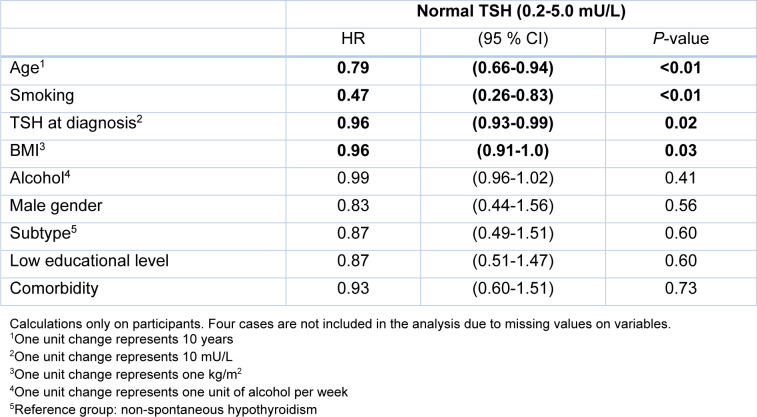
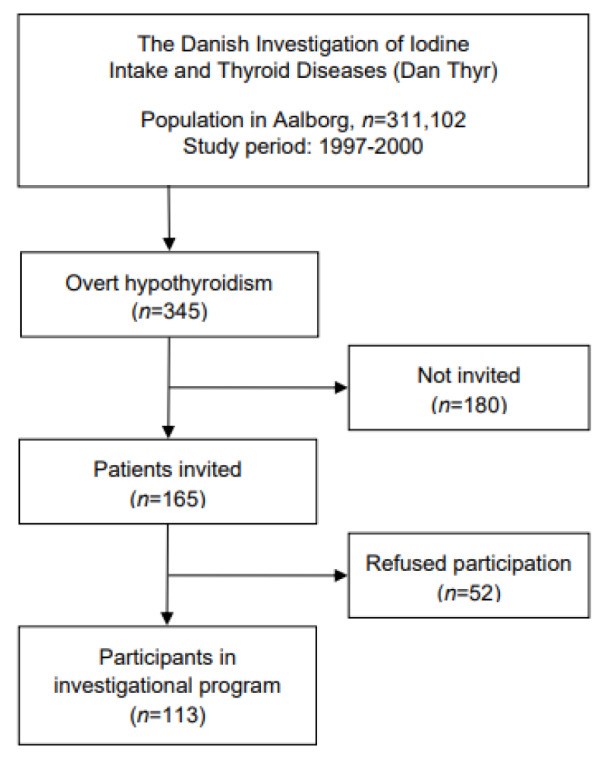
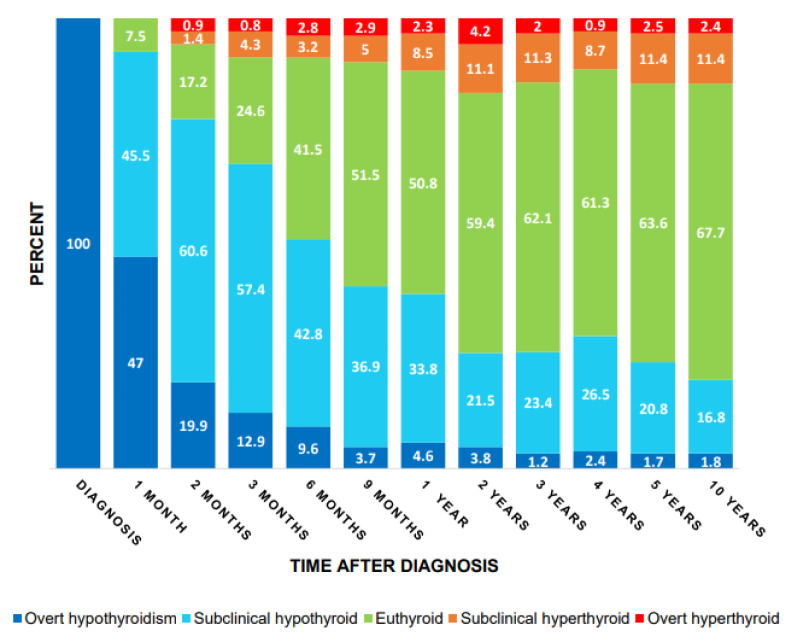
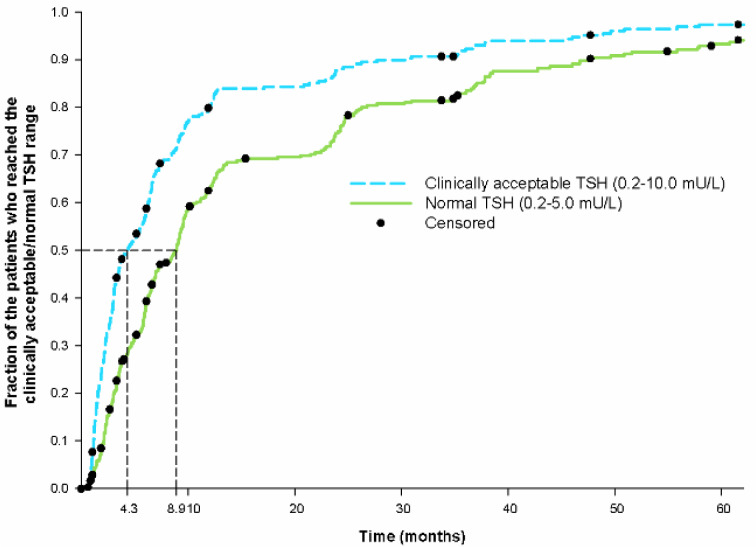
The aim of this study is to evaluate the adequacy of treatment, and to identify factors influencing treatment of hypothyroidism. Patients newly diagnosed with overt hypothyroidism (n=345) were identified via a register linked to a laboratory database. In selected periods with staff available, 165 patients were invited, and 113 (68.5 %) accepted participating in a comprehensive program including blood tests and completion of questionnaires. We performed a longitudinal follow-up on thyroid function tests 10 years after the diagnosis. Time to reach a serum TSH level of 0.2-10 mU/L (termed as clinically acceptable) and biochemical normalization (TSH: 0.2-5.0 mU/L), respectively, were analyzed using Kaplan Meier survival analysis. Predictors for longer duration to reach the normal TSH range were identified using cox proportional hazards regression. Only 67.7 % of the patients were in the euthyroid range on the long term after diagnosis of overt hypothyroidism (2 years: 59.4 %; 10 years: 67.7 %). Median time to the first normal TSH was 8.9 months (95 % CI: 7.6-10.2 months). The factors associated with longer duration until normalization of TSH after multivariate analysis were age (HR 0.79 per 10 years; 95 % CI: 0.66-0.94; P = <0.01), smoking (HR 0.47; 95 % CI: 0.26-0.83; P = <0.01), serum TSH at diagnosis (HR 0.96 per 10 mU/L; 95 % CI: 0.93-0.99; P = 0.02) and BMI (HR 0.96 per kg/m2; 95 % CI: 0.91-0.99; P = 0.03). A considerable number of hypothyroid patients remained inadequately treated. When treating hypothyroid patients, special attention should be addressed to those patients who never or lately obtain euthyroid status.
Keywords: hypothyroidism; overt hypothyroidism; population-based study; treatment.
Copyright © 2022 Lindgård Nielsen et al.
Figures
Similar articles
-
Over- and Under-Treatment of Hypothyroidism Is Associated with Excess Mortality: A Register-Based Cohort Study.Thyroid. 2018 May;28(5):566-574. doi: 10.1089/thy.2017.0517. Epub 2018 Apr 26. Thyroid. 2018. PMID: 29631518
-
Spontaneous subclinical hypothyroidism in patients older than 55 years: an analysis of natural course and risk factors for the development of overt thyroid failure.J Clin Endocrinol Metab. 2004 Oct;89(10):4890-7. doi: 10.1210/jc.2003-032061. J Clin Endocrinol Metab. 2004. PMID: 15472181
-
Duration of thyroid dysfunction correlates with all-cause mortality. the OPENTHYRO Register Cohort.PLoS One. 2014 Oct 23;9(10):e110437. doi: 10.1371/journal.pone.0110437. eCollection 2014. PLoS One. 2014. PMID: 25340819 Free PMC article.
-
Endemic infantile hypothyroidism in a severe endemic goitre area of central Africa.Clin Endocrinol (Oxf). 1984 Mar;20(3):327-40. doi: 10.1111/j.1365-2265.1984.tb00089.x. Clin Endocrinol (Oxf). 1984. PMID: 6723080
-
The Stability of TSH, and Thyroid Hormones, in Patients Treated With Tablet, or Liquid Levo-Thyroxine.Front Endocrinol (Lausanne). 2021 Mar 10;12:633587. doi: 10.3389/fendo.2021.633587. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 33790863 Free PMC article. Review.
Cited by
-
The Impact of Hypothyroidism on Cardiovascular-Related Healthcare Utilization in the US Population With Diabetes.J Endocr Soc. 2024 Nov 18;9(1):bvae204. doi: 10.1210/jendso/bvae204. eCollection 2024 Nov 26. J Endocr Soc. 2024. PMID: 39669655 Free PMC article.
-
TSH Trajectories During Levothyroxine Treatment in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) Cohort.J Clin Endocrinol Metab. 2024 Nov 18;109(12):3065-3075. doi: 10.1210/clinem/dgae294. J Clin Endocrinol Metab. 2024. PMID: 38780968 Free PMC article.
-
Thyroid function status in patients with hypothyroidism on thyroxine replacement and associated factors: a retrospective cohort study in primary care.BMC Prim Care. 2024 Oct 26;25(1):383. doi: 10.1186/s12875-024-02613-z. BMC Prim Care. 2024. PMID: 39462347 Free PMC article.
-
Long-term outcomes of LT4/LT3 combination treatment for persistent hypothyroid symptoms.Eur Thyroid J. 2025 Mar 4;14(2):e240275. doi: 10.1530/ETJ-24-0275. Print 2025 Apr 1. Eur Thyroid J. 2025. PMID: 39982807 Free PMC article.
-
Phase 1 Study Evaluating the Pharmacokinetics, Dose Proportionality, Bioavailability, and Tolerability of Subcutaneous Levothyroxine Sodium (XP-8121).Clin Transl Sci. 2025 May;18(5):e70244. doi: 10.1111/cts.70244. Clin Transl Sci. 2025. PMID: 40348586 Free PMC article. Clinical Trial.
References
-
- Canaris GJ, Manowitz NR, Mayor G, Ridgway EC. The colorado thyroid disease prevalence study. Arch Intern Med. 2000;160:526–34. - PubMed
-
- Carlé A, Bülow Pedersen I, Knudsen N, Perrild H, Ovesen L, Laurberg P. Gender differences in symptoms of hypothyroidism: A population-based DanThyr study. Clin Endocrinol (Oxf) 2015;83:717–25. - PubMed
-
- Carlé A, Laurberg P, Knudsen N, Perrild H, Ovesen L, Rasmussen LB, et al. Thyroid peroxidase and thyroglobulin auto-antibodies in patients with newly diagnosed overt hypothyroidism. Autoimmunity. 2006;39:497–503. - PubMed
-
- Carlé A, Laurberg P, Pedersen IB, Knudsen N, Perrild H, Ovesen L, et al. Epidemiology of subtypes of hypothyroidism in Denmark. Eur J Endocrinol. 2006;154:21–8. - PubMed
-
- Carlé A, Laurberg P, Pedersen IB, Knudsen N, Perrild H, Ovesen L, et al. Mainly the younger hypothyroid patients are referred to hospital - Evidence for referral bias. J Clin Epidemiol. 2009;62:446–51. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials