

Durable strong efficacy and favorable long-term renal safety of the anatomically optimized distal renal denervation according to the 3 year follow-up extension of the double-blind randomized controlled trial
- PMID: 35146146
- PMCID: PMC8819529
- DOI: 10.1016/j.heliyon.2022.e08747
Durable strong efficacy and favorable long-term renal safety of the anatomically optimized distal renal denervation according to the 3 year follow-up extension of the double-blind randomized controlled trial
Abstract
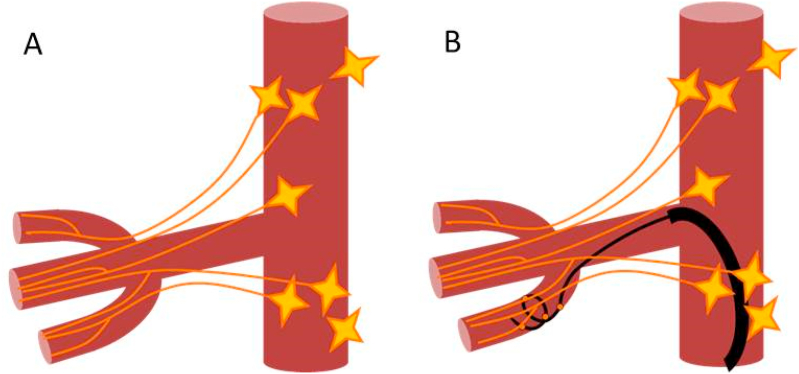
Background: Historical reports on surgical renal denervation consistently describe renal plexus as a triangle or fan-like structure converging at the kidney gate. Following that anatomy, we developed a distal mode of radiofrequency renal denervation (RDN) mainly in segmental branches of the renal artery and confirmed its superior efficacy over the conventional main trunk procedure in a 6-months double-blind randomized controlled trial (NCT02667912). To assess the long-term effects of distal RDN we extended the follow-up of our study to three years.
Methods: BP, serum creatinine, eGFR were measured one and three years after randomization; major adverse renal events were assessed over the entire study period. The blinding was maintained over the entire three-year study period.
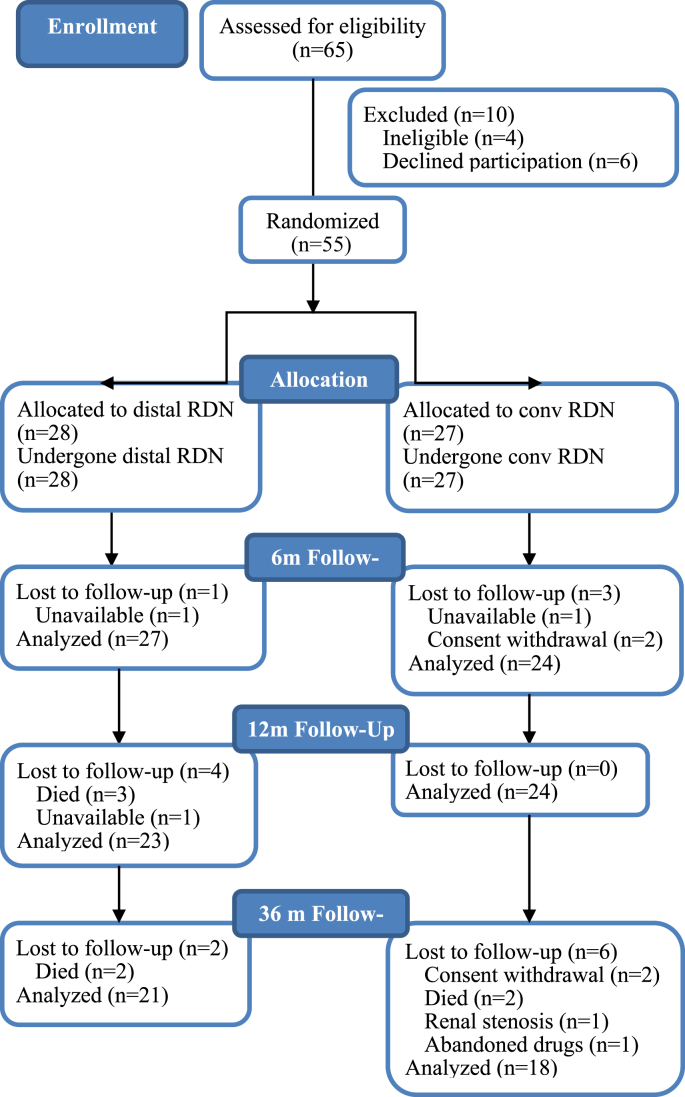
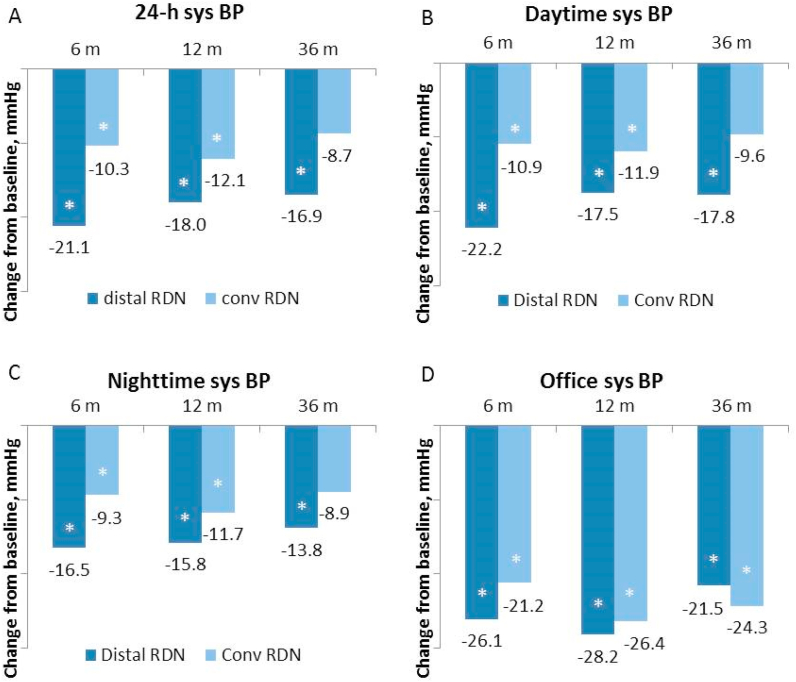
Findings: Of 55 randomized patients, 47 (23/24, distal/main trunk RDN, respectively) were assessed at one year and 39 (21/18) at three years post-procedure. Twenty-four-hour ambulatory systolic BP remained powerfully lowered after distal RDN both at one- and three-years assessments(mean change from baseline: -18.0, 95% CI -27.6 to -8.5; p<0.05 and -16·9, 95% CI -27·3 to -6·5; p<0·05, mmHg, respectively. This was accompanied by a moderate drop in eGFR at one year: -8·9 ml/min/m2, 95% CI -14·8 to -3·1; p<0·05, which, however, subsequently decreased in size at three years: -6·5, 95% CI -13·2 to 0·3; p>0·05. After main trunk RDN, the decrease of 24h systolic BP was quite moderate at one year: -12·1, 95% CI -19·2 to -5·0; p<0·05, and further weakened at three-year assessment: -8·5, 95% CI -19·7 to 2·2; p>0.05. eGFR was almost unchanged at one year: -1·3, 95% CI -6·6 to 4·0; p>0·05, but significantly decreased at three years: -5·0, 95% CI -9·6 to -0·3; p<0·05.
Interpretation: Our data demonstrate the durable strong BP-lowering efficacy and favorable long-term renal safety of distal RDN.
Keywords: Ambulatory; Arterial catheterization; Blood pressure monitoring; Essential hypertension; Peripheral; Radiofrequency ablation; Renal artery.
© 2022 The Authors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Morrissey D.M., Brookes VictorS., Cooke W.T. Sympathectomy in the treatment of hypertension review of 122 cases. Lancet. 1953;261(6757) https://www.sciencedirect.com/science/article/pii/S014067365391589X 403-408, ISSN 0140-6736. - PubMed
-
- Smithwick R.H., Thompson J.E. Splanchnicectomy for essential hypertension: results in 1,266 cases. JAMA. 1953;152(16):1501–1504. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
