

Secondary vitreoretinal lymphoma with spontaneous regression
- PMID: 35146209
- PMCID: PMC8818703
- DOI: 10.1016/j.ajoc.2022.101357
Secondary vitreoretinal lymphoma with spontaneous regression
Abstract
Purpose: To report a patient with vitreoretinal lymphoma (VRL) secondary to systemic diffuse large B-cell lymphoma, who had two episodes of spontaneous regression.
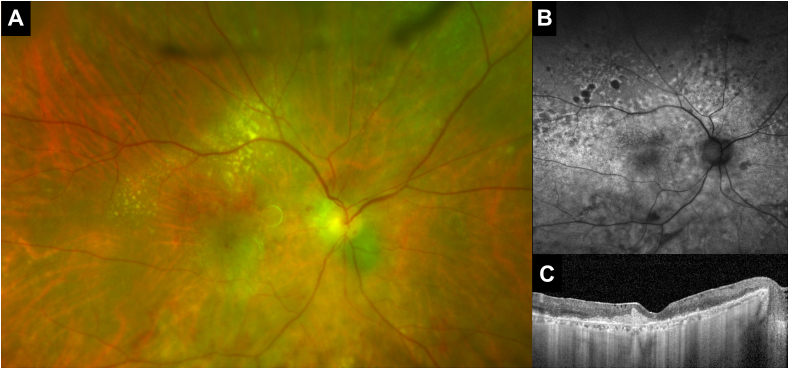
Observations: An 80-year-old Nicaraguan male with a history of treated systemic diffuse large B-cell lymphoma presented with decreased vision in his right eye over one year. The patient was found to have subretinal lesions and moderate vitreous opacities in his right eye. Cytological analysis of vitreous confirmed B-cell lymphoma. Following his systemic work-up, spontaneous clinical improvement was noted. There were no vitreoretinal or systemic lymphoma recurrences during one year of follow-up until the patient had new onset decreased vision in the left eye. He was presumed to have a recurrence of VRL supported by optical coherence tomography findings. Repeat systemic workup was negative for reoccurrence and the ocular lesions resolved spontaneously over 4 weeks.
Conclusions: Spontaneous regression of intraocular lymphoma can rarely occur. Multimodal imaging has an essential role in diagnosing and monitoring recurrence of this disease.
Keywords: Large B-cell lymphoma; Multimodal imaging; Recurrence; Spontaneous regression; Vitreoretinal lymphoma.
© 2022 Published by Elsevier Inc.
Conflict of interest statement
The following authors have no financial disclosures: WK, AK, JS, HW, HNS, SK.
Figures


Similar articles
-
Spontaneous regression of secondary vitreoretinal lymphoma after diagnostic vitrectomy: case report.BMC Ophthalmol. 2023 May 17;23(1):222. doi: 10.1186/s12886-023-02967-5. BMC Ophthalmol. 2023. PMID: 37198561 Free PMC article.
-
Vitreoretinal presentation of secondary large B-cell lymphoma in patients with systemic lymphoma.JAMA Ophthalmol. 2013 Sep;131(9):1151-8. doi: 10.1001/jamaophthalmol.2013.334. JAMA Ophthalmol. 2013. PMID: 23744124
-
Multimodal imaging in a case of presumed secondary vitreoretinal lymphoma presenting with inner retina and optic nerve head infiltration.Am J Ophthalmol Case Rep. 2024 Mar 11;34:102040. doi: 10.1016/j.ajoc.2024.102040. eCollection 2024 Jun. Am J Ophthalmol Case Rep. 2024. PMID: 38532849 Free PMC article.
-
Challenges in the diagnosis and management of vitreoretinal lymphoma - Clinical and basic approaches.Prog Retin Eye Res. 2022 Sep;90:101053. doi: 10.1016/j.preteyeres.2022.101053. Epub 2022 Feb 21. Prog Retin Eye Res. 2022. PMID: 35210172 Review.
-
Clinical guidelines for the diagnosis and treatment of vitreoretinal lymphoma in Chinese patients (2024).Eye Vis (Lond). 2025 May 26;12(1):20. doi: 10.1186/s40662-025-00434-4. Eye Vis (Lond). 2025. PMID: 40414948 Free PMC article. Review.
Cited by
-
Diagnosis of Secondary Vitreoretinal Lymphoma With Neurosurgical Stereotactic Biopsy: A Multimodal Diagnostic and Imaging Approach.J Vitreoretin Dis. 2025 Jul 14:24741264251356295. doi: 10.1177/24741264251356295. Online ahead of print. J Vitreoretin Dis. 2025. PMID: 40672690 Free PMC article.
-
Electroretinographic and Optical Coherence Tomographic Evaluations of Eyes with Vitreoretinal Lymphoma.J Clin Med. 2023 Jun 9;12(12):3957. doi: 10.3390/jcm12123957. J Clin Med. 2023. PMID: 37373651 Free PMC article.
-
Spontaneous regression of secondary vitreoretinal lymphoma after diagnostic vitrectomy: case report.BMC Ophthalmol. 2023 May 17;23(1):222. doi: 10.1186/s12886-023-02967-5. BMC Ophthalmol. 2023. PMID: 37198561 Free PMC article.
References
-
- Levasseur S.D., Wittenberg L.A., White V.A. Vitreoretinal lymphoma: a 20-year review of incidence, clinical and cytologic features, treatment, and outcomes. JAMA Ophthalmol. 2013;131(1):50–55. - PubMed
-
- Fend F., Ferreri A.J.M., Coupland S.E. How we diagnose and treat vitreoretinal lymphoma. Br J Haematol. 2016;173(5):680–692. - PubMed
-
- Mashayekhi A., Dalvin L.A., Lim L.-A.S., et al. Association of vitreoretinal lymphoma with systemic lymphoma. Retina. 2021;41(2):259–265. - PubMed
-
- Stanoszek L.M., Smith L.B., Grajewski K., Reneau J.C., Wilcox R., Perry A.M. Spontaneous regression of high-grade B-cell lymphoma with MYC and BCL2 rearrangements: case report and literature review. Clin Lymphoma, Myeloma & Leukemia. 2021;21(2):e120–e125. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
