

A case of Epstein-Barr virus acute retinal necrosis successfully treated with foscarnet
- PMID: 35146210
- PMCID: PMC8818534
- DOI: 10.1016/j.ajoc.2022.101363
A case of Epstein-Barr virus acute retinal necrosis successfully treated with foscarnet
Abstract
Purpose: Epstein-Barr virus (EBV) is a herpes virus known to cause infectious mononucleosis and several other human disorders. Ocular EBV infections that have been reported include uveitis, retinal vasculitis, and acute retinal necrosis (ARN). ARN is usually caused by herpes simplex virus (HSV) or varicella-zoster virus (VZV). ARN that is caused by EBV (EBV-ARN) is rarely seen, and only a few cases have been reported. The visual prognosis for EBV-ARN is poor, and no treatment strategy has been established. We report on a patient who was treated successfully for EBV-ARN.
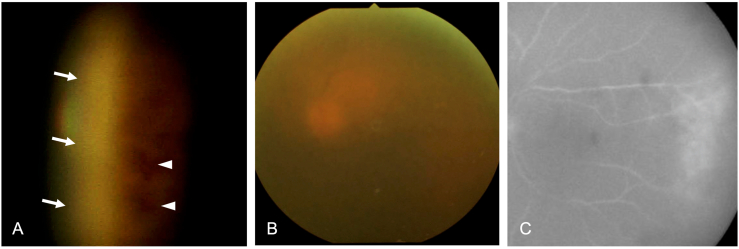
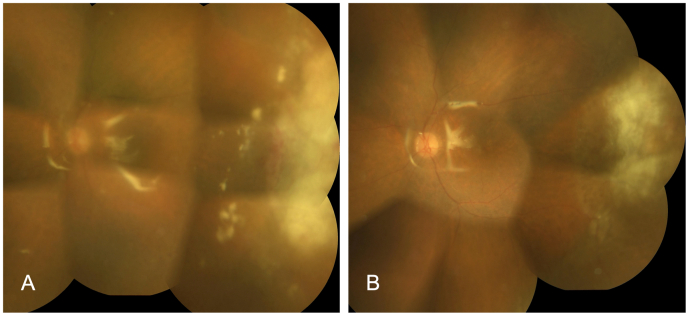
Observation: An 80-year-old female who had been treated with prednisolone at 5 mg/day and methotrexate at 2 mg/week for rheumatoid arthritis visited our hospital because of blurred vision in her left eye. Her left visual acuity was 20/50, and extensive white-yellowish retinal lesions at the temporal periphery with retinal hemorrhages were seen through vitreous haze. The DNA sequence of EBV, but not of HSV, VZV, or cytomegalovirus, was detected by a polymerase chain reaction (PCR) assay in the aqueous humor (4.2 × 106 copies/ml), with EBV also being positive in serum (3.5 × 102 copies/ml). The patient received 2 mg of intravitreal ganciclovir injections twice with a 3-day interval and intravenous infusion of acyclovir at 750 mg/day for 7 days; however, the retinal white lesions expanded rapidly, then dose of prednisolone was increased (40 mg/day) and vitrectomy was performed 10 days after the initial visit. After the surgery, the retinal lesion continued to enlarge. Vitreous samples showed high copies of EBV (1.2 × 108 copies/ml). Following treatment with intravenous foscarnet (4800 mg/day), which replaced the acyclovir application, the retinal white lesions gradually diminished, leaving retinal scars. To date, the patient has developed no retinal detachment and shows visual acuity over 6/60 in the left eye along with silicone oil.
Conclusions: We experienced a case of EBV-ARN that was refractory to systemic acyclovir and topical ganciclovir but responded effectively to systemic foscarnet after vitrectomy. Although the clinical management remains challenging in this disease, foscarnet is considered to be one of the candidate drugs for EBV infections.
Keywords: ARN, acute retinal necrosis; Acute retinal necrosis; Acyclovir; CMV, cytomegalovirus; EBV, Epstein-Barr virus; EBV-ARN, ARN caused by EBV; Epstein-Barr virus; Foscarnet; Ganciclovir; HSV, herpes simplex virus; PCR, polymerase chain reaction; Polymerase chain reaction; VZV, varicella-zoster virus.
© 2022 The Authors.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Acute Retinal Necrosis Associated with Epstein-Barr Virus in a Patient Undergoing Immunosuppressive Therapy.Case Rep Ophthalmol. 2016 Apr 12;7(1):195-201. doi: 10.1159/000445372. eCollection 2016 Jan-Apr. Case Rep Ophthalmol. 2016. PMID: 27194989 Free PMC article.
-
Acute retinal necrosis: the effects of intravitreal foscarnet and virus type on outcome.Ophthalmology. 2010 Mar;117(3):556-60. doi: 10.1016/j.ophtha.2009.08.003. Epub 2009 Dec 23. Ophthalmology. 2010. PMID: 20031221
-
Acute retinal necrosis.Semin Ophthalmol. 2005 Jul-Sep;20(3):155-60. doi: 10.1080/08820530500232027. Semin Ophthalmol. 2005. PMID: 16282149 Review.
-
Treatment of Refractory Acute Retinal Necrosis with Intravenous Foscarnet or Cidofovir.Ocul Immunol Inflamm. 2018;26(2):199-203. doi: 10.1080/09273948.2016.1207788. Epub 2016 Sep 6. Ocul Immunol Inflamm. 2018. PMID: 27598973
-
EPSTEIN-BARR VIRUS ACUTE RETINAL NECROSIS IN AN IMMUNOCOMPETENT HOST.Retin Cases Brief Rep. 2021 Jul 1;15(4):412-416. doi: 10.1097/ICB.0000000000000819. Retin Cases Brief Rep. 2021. PMID: 30358736 Review.
Cited by
-
Clinical characteristics and outcomes of acute retinal necrosis at different stages: a retrospective study.BMC Ophthalmol. 2025 Mar 4;25(1):107. doi: 10.1186/s12886-025-03937-9. BMC Ophthalmol. 2025. PMID: 40038654 Free PMC article.
-
Repurposing Licensed Drugs with Activity Against Epstein-Barr Virus for Treatment of Multiple Sclerosis: A Systematic Approach.CNS Drugs. 2025 Mar;39(3):305-320. doi: 10.1007/s40263-024-01153-5. Epub 2025 Jan 10. CNS Drugs. 2025. PMID: 39792343
-
Successful treatment of Keratitis caused by Mycobacterium chelonae and an overview of previous cases in Europe.Ann Clin Microbiol Antimicrob. 2024 Oct 9;23(1):92. doi: 10.1186/s12941-024-00752-w. Ann Clin Microbiol Antimicrob. 2024. PMID: 39385246 Free PMC article. Review.
-
Primary treatment failure in acute retinal necrosis - A comprehensive review.Indian J Ophthalmol. 2024 Dec 1;72(12):1694-1703. doi: 10.4103/IJO.IJO_689_24. Epub 2024 Aug 14. Indian J Ophthalmol. 2024. PMID: 39186630 Free PMC article. Review.
-
Acute retinal necrosis: A mini review.Front Ophthalmol (Lausanne). 2022 Aug 22;2:916113. doi: 10.3389/fopht.2022.916113. eCollection 2022. Front Ophthalmol (Lausanne). 2022. PMID: 38983554 Free PMC article. Review.
References
-
- Lau C.H., Missotten T., Salzmann J., Lightman S.L. Acute retinal necrosis features, management, and outcomes. Ophthalmology. 2007;114:756–762. - PubMed
-
- Hillenkamp J., Nölle B., Bruns C., Rautenberg P., Fickenscher H., Roider J. Acute retinal necrosis: clinical features, early vitrectomy, and outcomes. Ophthalmology. 2009;116 1971-5.e2. - PubMed
-
- Grossniklaus H.E., Aaberg T.M., Purnell E.W., Luka J., Seemayer T.A. Retinal necrosis in X-linked lymphoproliferative disease. Ophthalmology. 1994;101:705–709. - PubMed
-
- Hershberger V.S., Hutchins R.K., Witte D.P., Schneider S., Harris R.E., McGonegle S.J. Epstein-Barr virus-related bilateral acute retinal necrosis in a patient with X-linked lymphoproliferative disorder. Arch Ophthalmol. 2003;121:1047–1049. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
