

Neglected and (re-)emergent infections of the CNS i n low-/middle-income countries
- PMID: 35146359
- PMCID: PMC8805465
- DOI: 10.53854/liim-2904-3
Neglected and (re-)emergent infections of the CNS i n low-/middle-income countries
Abstract
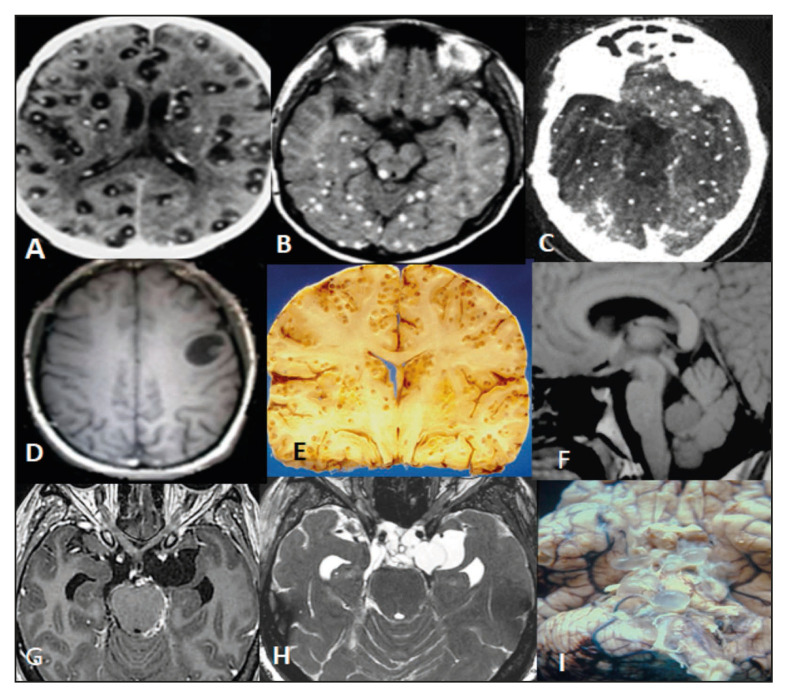
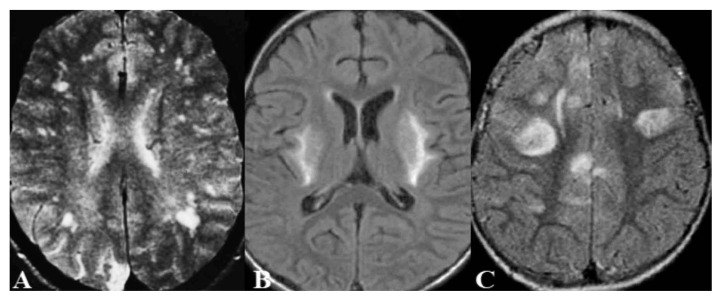
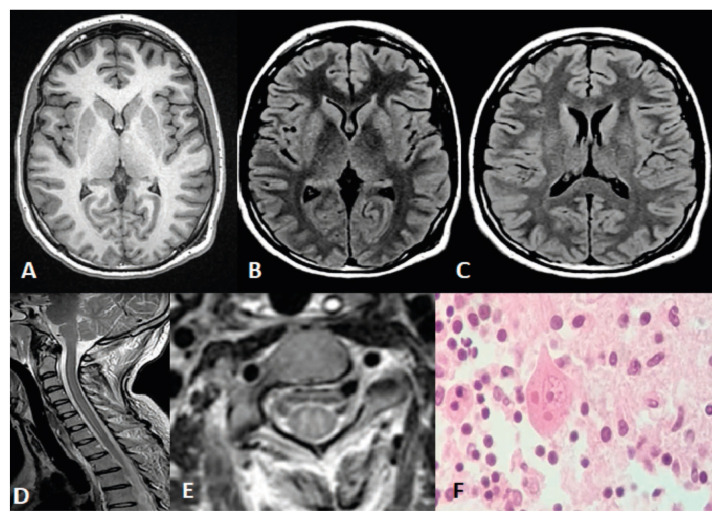
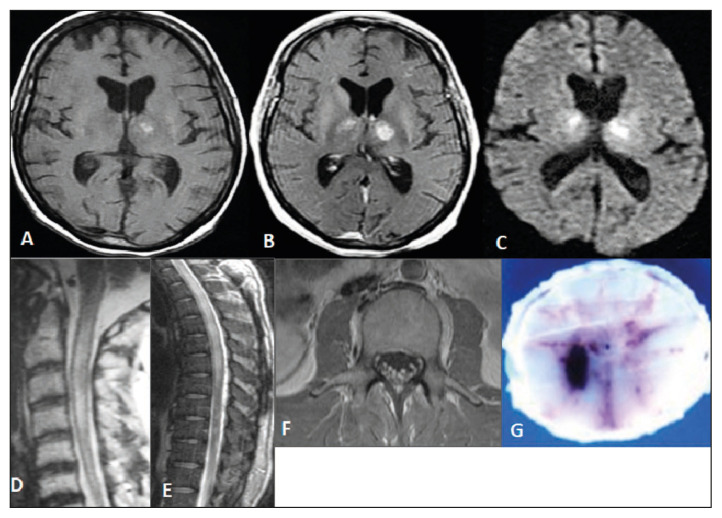
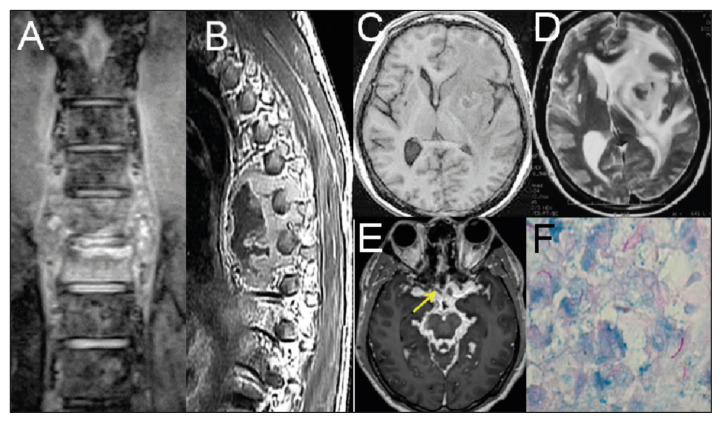
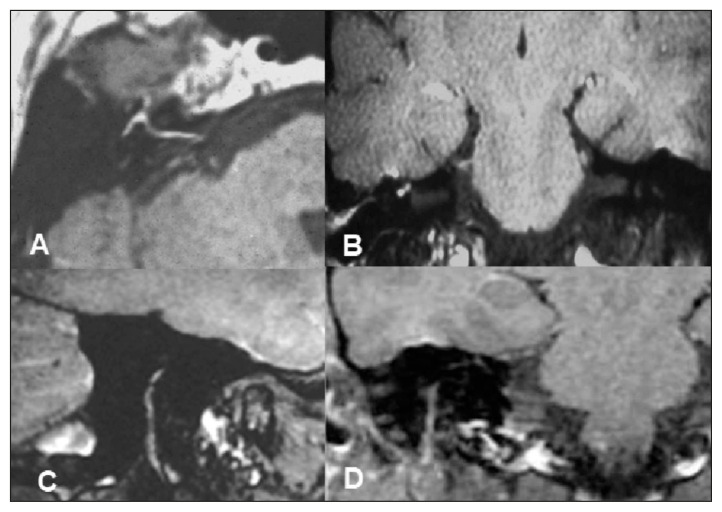
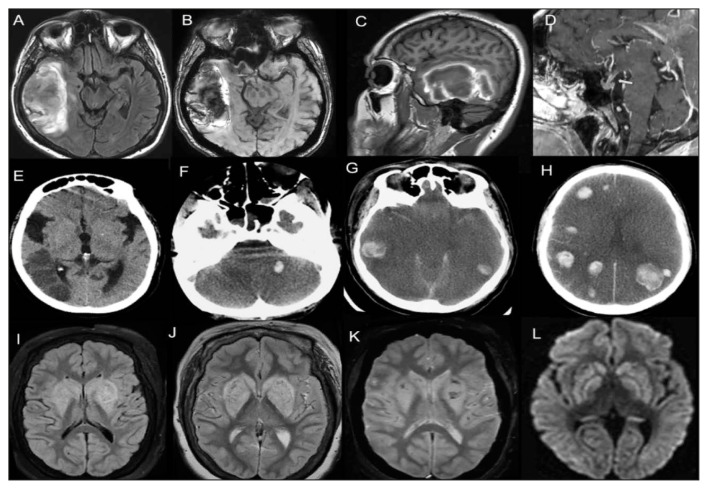
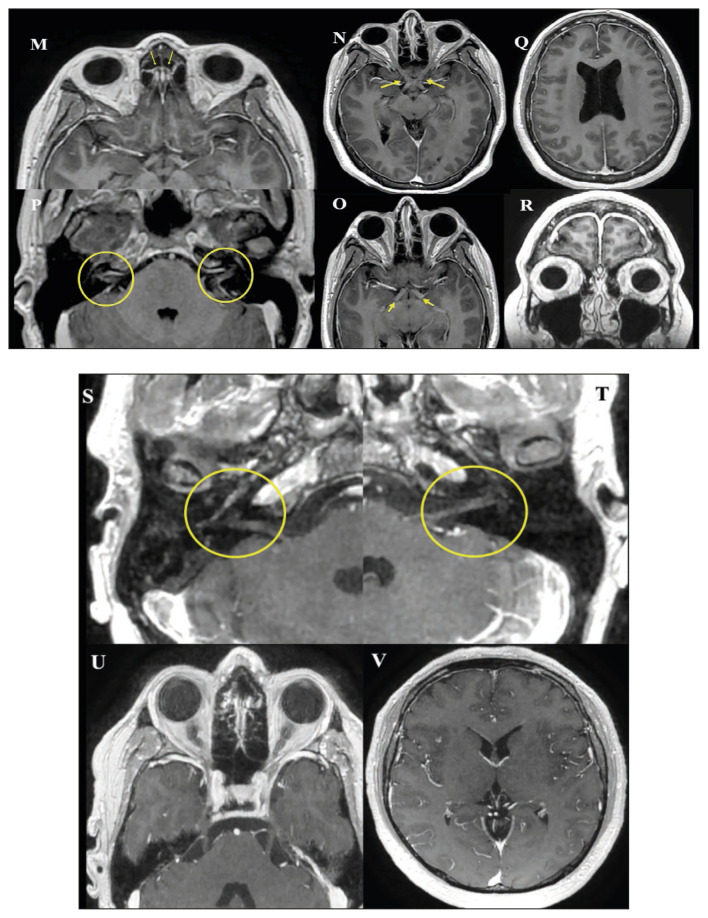
Low- and middle-income countries (LMIC) have suffered from long-term health system deficiencies, worsened by poor living conditions, lack of sanitation, a restricted access to health facilities and running water, overcrowding, and overpopulation. These factors favor human displacement and deepen marginalization; consequently, their population endures a high burden of infectious diseases. In this context, the current epidemiological landscape and its impact on health and economic development are not promissory, despite the commitment by the international community to eradicate neglected tropical infections - especially tuberculosis and malaria, by 2030. Neglected and (re)-emerging infectious diseases affecting the central nervous system (CNS) are a major public health concern in these countries, as they cause a great morbidity and mortality; furthermore, survivors often suffer from severe neurological disabilities. Herein, we present a retrospective review focused on some neglected and (re)-emerging infectious diseases, including neurocysticercosis, malaria, rabies, West Nile virus encephalitis, tuberculosis, neuroborreliosis, and SARS-CoV-2 in LMIC. A retrospective review of studies on selected neglected and (re)-emerging infectious diseases in LMIC was performed, including reports by the World Health Organization (WHO) published within the last five years. Data on infection by SARS-CoV-2 were provided by the John Hopkins University Coronavirus Resource Center. CNS neglected and (re)-emerging infectious diseases remain as important causes of disease in LMIC. An alarming increase in the prevalence of malaria, tuberculosis, and cysticercosis is observed in the region, compounded by the recent COVID-19 pandemic. The WHO is currently supporting programs/efforts to cope with these diseases. Herein, we highlight the epidemiological burden of some CNS infections in LMIC, and their clinical and neuroimaging features, to facilitate an accurate diagnosis, considering that most of these diseases will not be eradicated in the short term; instead, their incidence will likely increase along with poverty, inequality, and related socioeconomic problems.
Keywords: Neglected; central nervous system; emergent; infections; low/middle income countries.
Copyright © 2016 - 2021 InfezMed.
Conflict of interest statement
Competing interests statement The authors declare that no conflict of interest exists.
Figures
References
-
- GBD 2016 DALY and HALE collaborators global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2012. A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1260–344. - PMC - PubMed
-
- World Population Ageing 2020 Highlights. [[accessed November 1, 2021].]. https://www.un.org/development/desa/pd/sites/www.un.org/development.desa... .
-
- World Population 2019. [[accessed November 1, 2021].]. At https://population.un.org/wpp/Publications/Files/WPP2019-wallchart.pdf.
-
- Kimura-Hayama ET, Higuera JA, Corona-Cedillo R, et al. Neurocysticercosis:radiologic-pathologic correlation. Radiographics. 2010;30(6):1705–19. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous