

Autologous haematopoietic stem cell transplantation versus low-dose immunosuppression in secondary-progressive multiple sclerosis
- PMID: 35146841
- PMCID: PMC9306891
- DOI: 10.1111/ene.15280
Autologous haematopoietic stem cell transplantation versus low-dose immunosuppression in secondary-progressive multiple sclerosis
Abstract
Background and purpose: Effectiveness of autologous haematopoietic stem cell transplantation (AHSCT) in relapsing-remitting multiple sclerosis (MS) is well known, but in secondary-progressive (SP)-MS it is still controversial. Therefore, AHSCT activity was evaluated in SP-MS using low-dose immunosuppression with cyclophosphamide (Cy) as a comparative treatment.
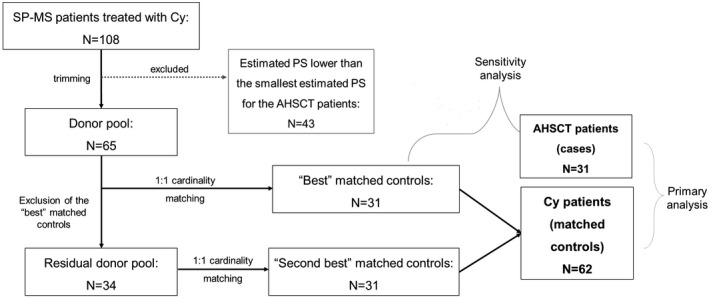
Methods: In this retrospective monocentric 1:2 matched study, SP-MS patients were treated with intermediate-intensity AHSCT (cases) or intravenous pulses of Cy (controls) at a single academic centre in Florence. Controls were selected according to baseline characteristics adopting cardinality matching after trimming on the estimated propensity score. Kaplan-Meier and Cox analyses were used to estimate survival free from relapses (R-FS), survival free from disability progression (P-FS), and no evidence of disease activity 2 (NEDA-2).
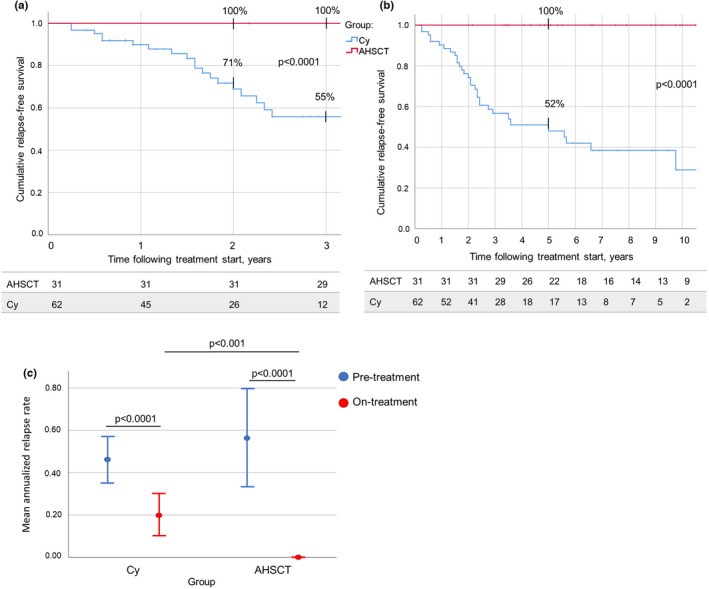
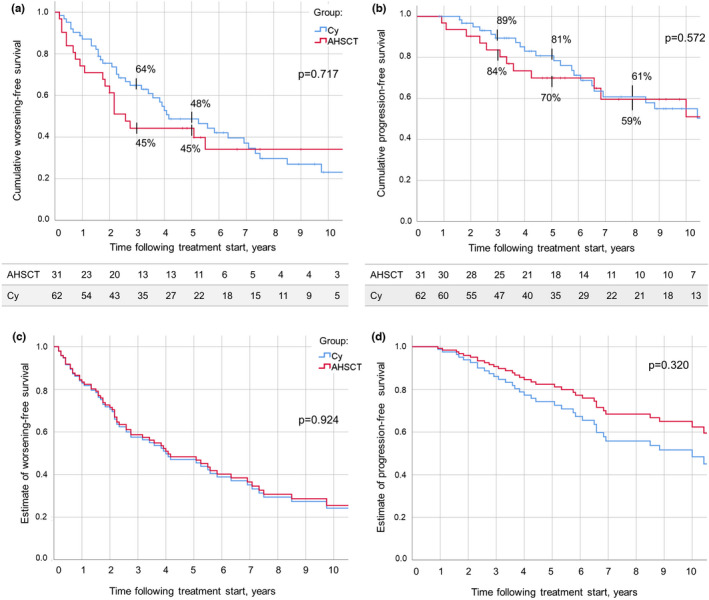
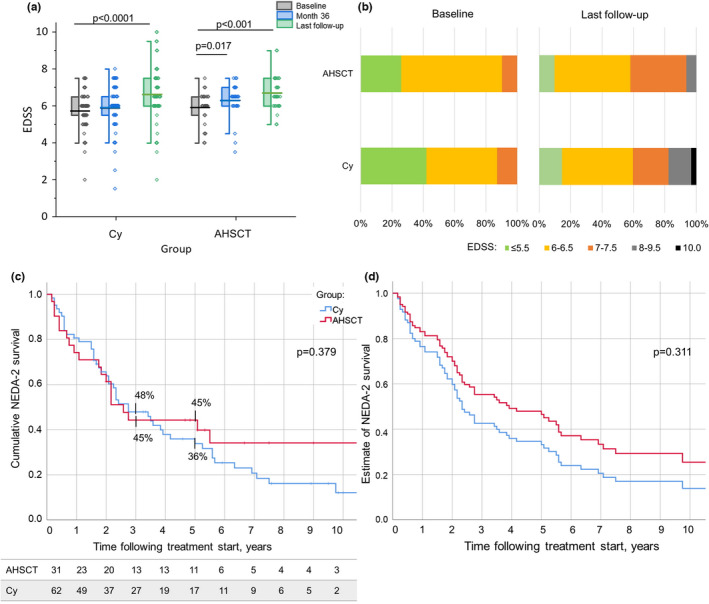
Results: A total of 93 SP-MS patients were included: 31 AHSCT, 62 Cy. Mean follow-up was 99 months in the AHSCT group and 91 months in the Cy group. R-FS was higher in AHSCT compared to Cy patients: at Year 5, 100% versus 52%, respectively (p < 0.0001). P-FS did not differ between the groups (at Year 5: 70% in AHSCT and 81% in Cy, p = 0.572), nor did NEDA-2 (p = 0.379). A sensitivity analysis including only the 31 "best-matched" controls confirmed these results. Three neoplasms (2 Cy, 1 AHSCT) and two fatalities (2 Cy) occurred.
Conclusions: This study provides Class III evidence, in SP-MS, on the superior effectiveness of AHSCT compared to Cy on relapse activity, without differences on disability accrual. Although the suppression of relapses was observed in the AHSCT group only, AHSCT did not show advantages over Cy on disability, suggesting that in SP-MS disability progression becomes based more on noninflammatory neurodegeneration than on inflammation.
Keywords: autologous hematopoietic stem cell transplantation; case-control study; disability progression; multiple sclerosis; progressive multiple sclerosis.
© 2022 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
A.Mar. reports nonfinancial support from Biogen Idec, Sanofi Genzyme, Novartis, Teva, and Roche, and personal fees from Merck Serono, outside the submitted work. A.M.R. has received personal compensation from Biogen Idec, Genzyme, Novartis, and Merck Serono for public speaking and advisory boards, outside the submitted work. R.S. reports honoraria from Jazz Pharmaceuticals and Sanofi Genzyme, outside the submitted work. L.M. has received educational grants and/or research funds from Fondazione Cassa di Risparmio di Firenze, Biogen, Merck Serono, Genzyme, and Roche and has received honoraria or consultation fees from Biogen, Roche, Mylan, Merck Serono, Genzyme, and Novartis, outside the submitted work. None of the other authors has any conflict of interest to disclose.
Figures
References
-
- Burt RK, Balabanov R, Burman J, et al. Effect of nonmyeloablative hematopoietic stem cell transplantation vs continued disease‐modifying therapy on disease progression in patients with relapsing‐remitting multiple sclerosis: a randomized clinical trial. JAMA. 2019;321:165‐174. 10.1001/jama.2018.18743 - DOI - PMC - PubMed
-
- Burt RK, Cohen BA, Russell E, et al. Hematopoietic stem cell transplantation for progressive multiple sclerosis: failure of a total body irradiation–based conditioning regimen to prevent disease progression in patients with high disability scores. Blood. 2003;102:2373‐2378. DOI: 10.1182/blood-2003-03-0877 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
