

DNAJC30 defect: a frequent cause of recessive Leber hereditary optic neuropathy and Leigh syndrome
- PMID: 35148383
- PMCID: PMC9166554
- DOI: 10.1093/brain/awac052
DNAJC30 defect: a frequent cause of recessive Leber hereditary optic neuropathy and Leigh syndrome
Abstract
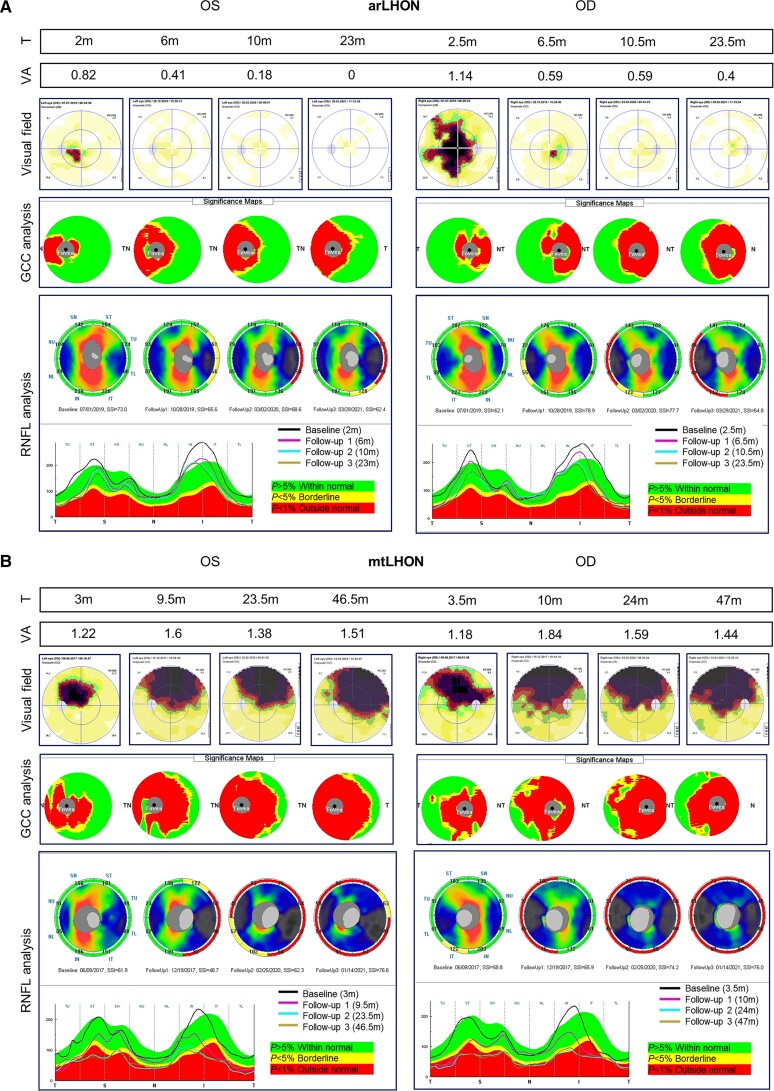
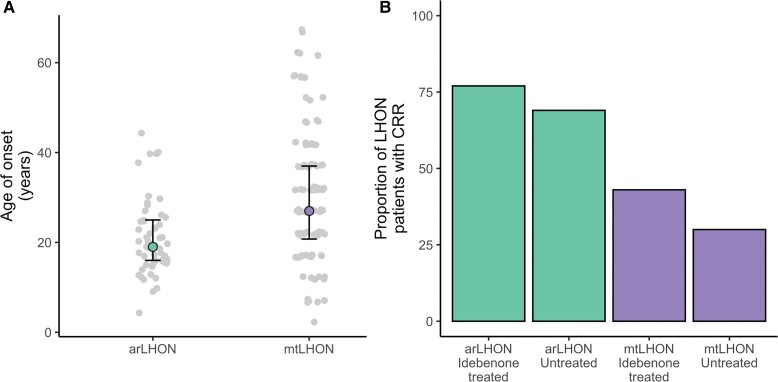
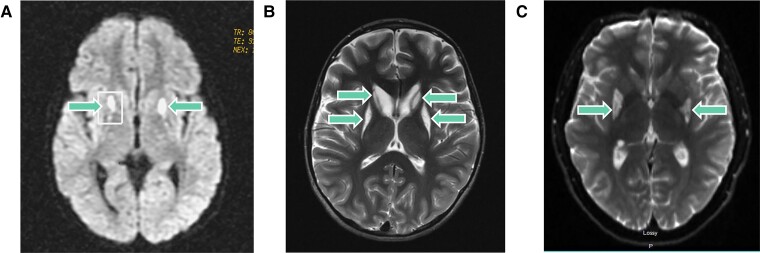
The recent description of biallelic DNAJC30 variants in Leber hereditary optic neuropathy (LHON) and Leigh syndrome challenged the longstanding assumption for LHON to be exclusively maternally inherited and broadened the genetic spectrum of Leigh syndrome, the most frequent paediatric mitochondrial disease. Herein, we characterize 28 so far unreported individuals from 26 families carrying a homozygous DNAJC30 p.Tyr51Cys founder variant, 24 manifesting with LHON, two manifesting with Leigh syndrome, and two remaining asymptomatic. This collection of unreported variant carriers confirms sex-dependent incomplete penetrance of the homozygous variant given a significant male predominance of disease and the report of asymptomatic homozygous variant carriers. The autosomal recessive LHON patients demonstrate an earlier age of disease onset and a higher rate of idebenone-treated and spontaneous recovery of vision in comparison to reported figures for maternally inherited disease. Moreover, the report of two additional patients with childhood- or adult-onset Leigh syndrome further evidences the association of DNAJC30 with Leigh syndrome, previously only reported in a single childhood-onset case.
Keywords: DNAJC30; LHON; Leigh syndrome; mitochondrial disease.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Carelli V, Carbonelli M, Irenaeus F, et al. International consensus statement on the clinical and therapeutic management of Leber hereditary optic neuropathy. J Neuroophthalmol. 2017;37(4):371–381. - PubMed
-
- Newman NJ. Treatment of hereditary optic neuropathies. Nat Rev Neurol. 2012;8(10):545–556. - PubMed
-
- Barboni P, Savini G, Valentino ML, et al. Leber’s hereditary optic neuropathy with childhood onset. Invest Ophthalmol Vis Sci. 2006;47(12):5303–5309. - PubMed
