

Relationship between time of emergency department admission and adherence to the Surviving Sepsis Campaign bundle in patients with septic shock
- PMID: 35148797
- PMCID: PMC8832860
- DOI: 10.1186/s13054-022-03899-0
Relationship between time of emergency department admission and adherence to the Surviving Sepsis Campaign bundle in patients with septic shock
Abstract
Background: Nighttime hospital admission is often associated with increased mortality risk in various diseases. This study investigated compliance rates with the Surviving Sepsis Campaign (SSC) 3-h bundle for daytime and nighttime emergency department (ED) admissions and the clinical impact of compliance on mortality in patients with septic shock.
Methods: We conducted an observational study using data from a prospective, multicenter registry for septic shock provided by the Korean Shock Society from 11 institutions from November 2015 to December 2017. The outcome was the compliance rate with the SSC 3-h bundle according to the time of arrival in the ED.
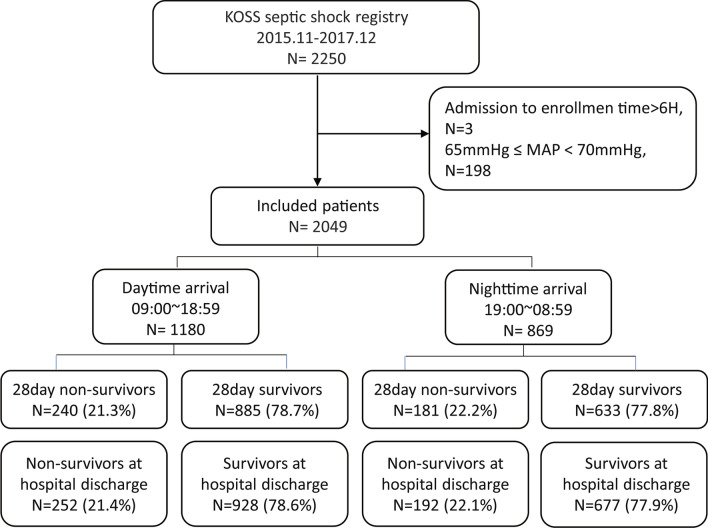
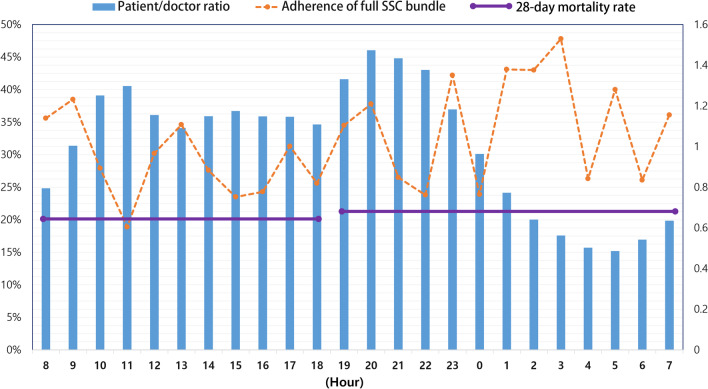
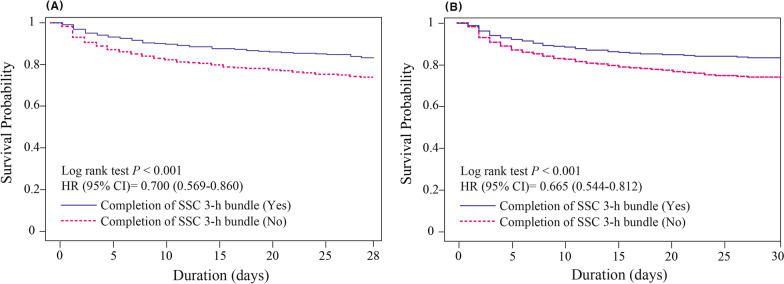
Results: A total of 2049 patients were enrolled. Compared with daytime admission, nighttime admission was associated with higher compliance with the administration of antibiotics within 3 h (adjusted odds ratio (adjOR), 1.326; 95% confidence interval (95% CI), 1.088-1.617, p = 0.005) and with the complete SSC bundle (adjOR, 1.368; 95% CI, 1.115-1.678; p = 0.003), likely to result from the increased volume of all patients and sepsis patients admitted during daytime hours. The hazard ratios of the completion of SSC bundle for 28-day mortality and in-hospital mortality were 0.750 (95% CI 0.590-0.952, p = 0.018) and 0.714 (95% CI 0.564-0.904, p = 0.005), respectively.
Conclusion: Septic shock patients admitted to the ED during the daytime exhibited lower sepsis bundle compliance than those admitted at night. Both the higher number of admitted patients and the higher patients to medical staff ratio during daytime may be factors that are responsible for lowering the compliance.
Keywords: Off-hour effect; Sepsis; Septic shock; Surviving Sepsis Campaign.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377. doi: 10.1007/s00134-017-4683-6. - DOI - PubMed
-
- Yang JM, Park YS, Chung SP, Chung HS, Lee HS, You JS, Lee SH, Park I. Implementation of a clinical pathway based on a computerized physician order entry system for ischemic stroke attenuates off-hour and weekend effects in the ED. Am J Emerg Med. 2014;32(8):884–889. doi: 10.1016/j.ajem.2014.04.049. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
