

CE: Assessing Movement-Evoked Pain
- PMID: 35149607
- PMCID: PMC11198877
- DOI: 10.1097/01.NAJ.0000822656.14887.1f
CE: Assessing Movement-Evoked Pain
Abstract
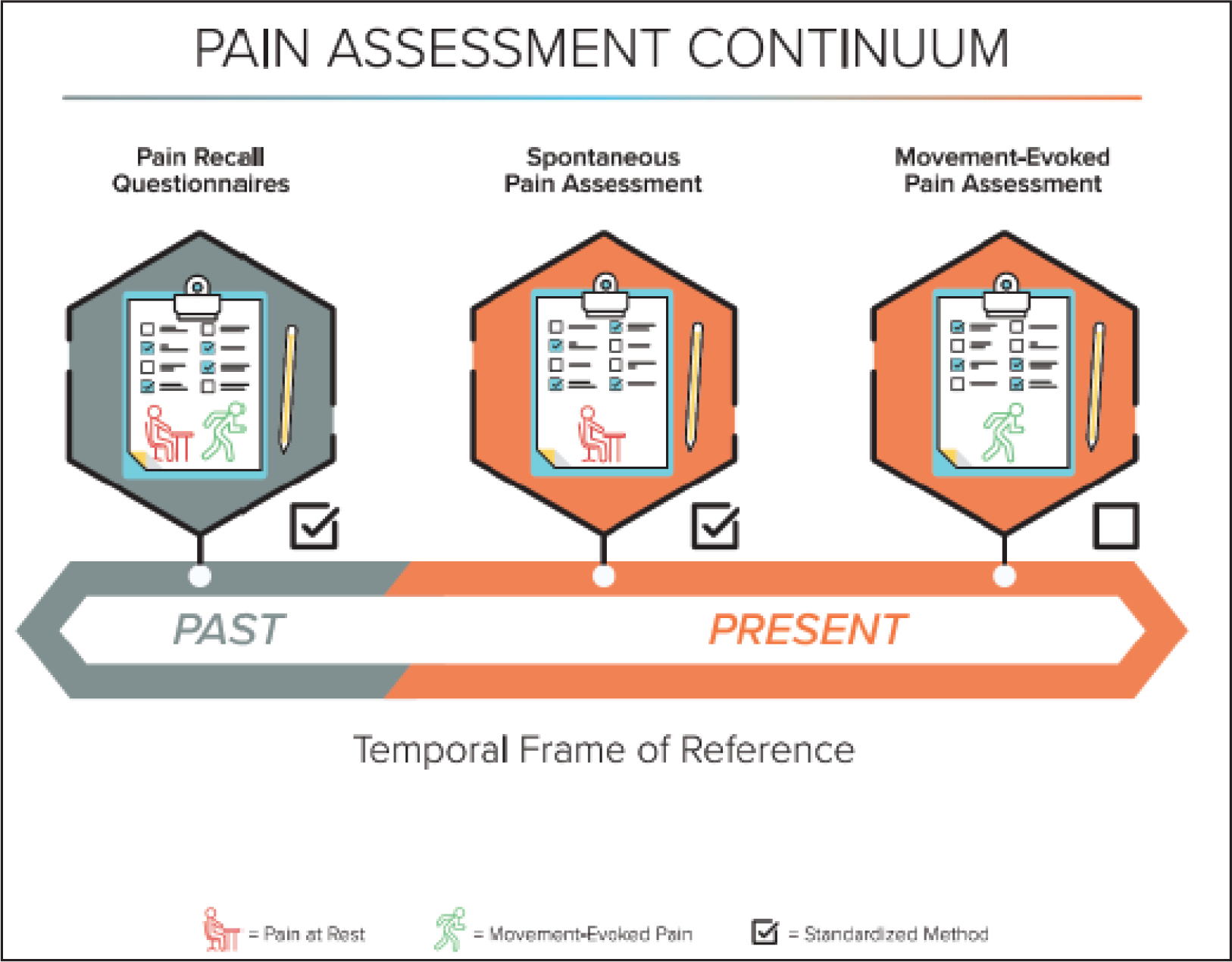
One of the most common and nuanced tasks that nurses perform is pain assessment, particularly in acute postoperative settings where frequent reassessments are needed. Most assessments are limited to obtaining a pain intensity score with little attention paid to the conditions necessitating the assessment or the factors contributing to the pain. Pain is frequently assessed during rest, but seldom during periods of movement or activity, which is a crucial omission given that acute postoperative movement-evoked pain (MEP) is intense and a common barrier to healing and restoration of function. In addition to physical limitations, MEP can impede cognitive, emotional, and social functioning in ways that can contribute to chronic pain, mood disorders, and disability. Professional and regulatory standards are moving away from a focus on pain intensity to an emphasis on its context, impact on function, and associated distress. Thus, there are many driving forces compelling nurses to integrate MEP assessments into practice to expedite the restoration of biopsychosocial functioning in postoperative patients. The authors discuss the clinical significance of a MEP assessment as well as protocols and tools for completing such assessments.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Disclosures: The authors report no actual or perceived conflicts of interests.
Figures
References
-
- Bischoff JM, Petersen M, Uçeyler N, Sommer C, Kehlet H, & Werner MU (2013). Lidocaine patch (5%) in treatment of persistent inguinal postherniorrhaphy pain: A randomized, double-blind, placebo-controlled, crossover trial. Anesthesiology, 119(6), 1444–1452. doi: 10.1097/ALN.0b013e3182a2a243. - DOI - PubMed
-
- Boitor M, Fiola JL, & Gélinas C (2016). Validation of the Critical-Care Pain Observation Tool and vital signs in relation to the sensory and affective components of pain during mediastinal tube removal in postoperative cardiac surgery intensive care unit adults. Journal of Cardiovascular Nursing, 31(5), 425–432. doi: 10.1097/JCN.0000000000000250. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
