

Adenoma characteristics associated with post-polypectomy proximal colon cancer incidence: a retrospective cohort study
- PMID: 35149853
- PMCID: PMC9174477
- DOI: 10.1038/s41416-022-01719-4
Adenoma characteristics associated with post-polypectomy proximal colon cancer incidence: a retrospective cohort study
Abstract
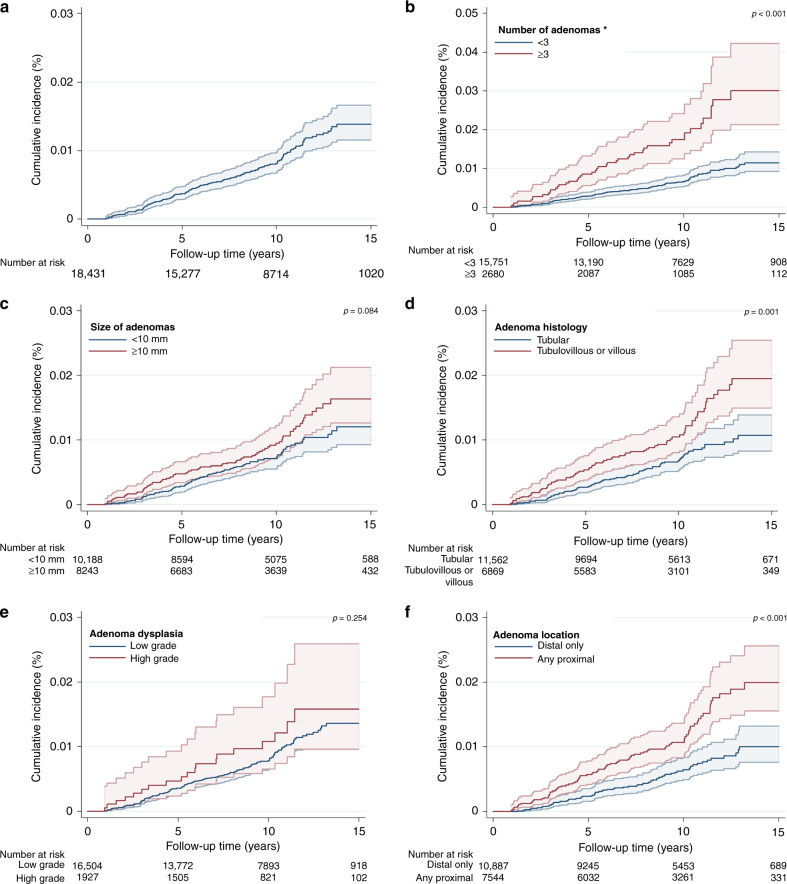
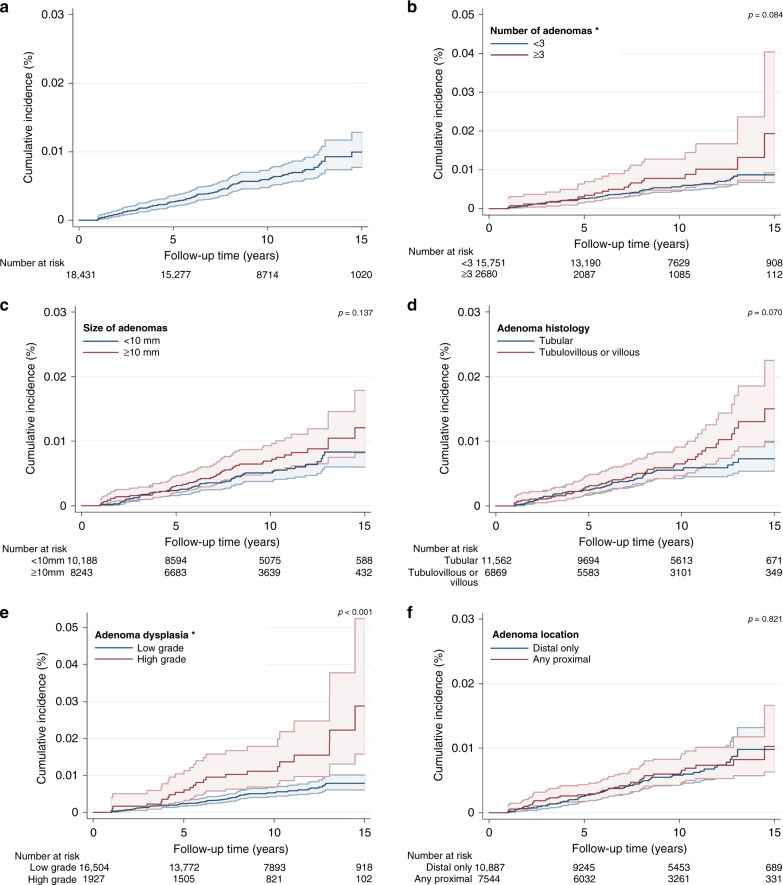
Background: Colorectal cancer (CRC) screening is less effective at reducing cancer incidence in the proximal colon compared to the distal colorectum. We aimed to identify adenoma characteristics associated with proximal colon cancer (PCC).
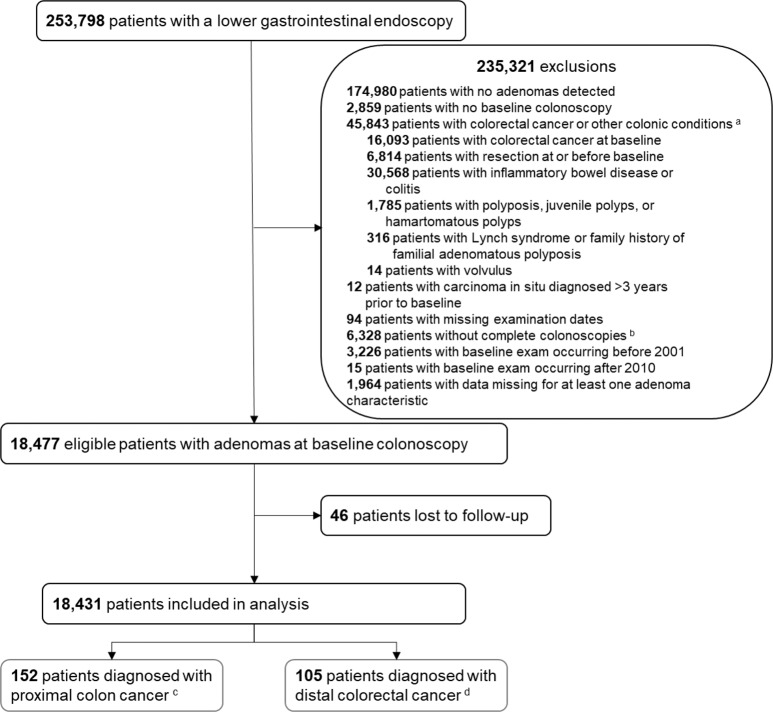
Methods: Endoscopy and pathology data for patients with ≥1 adenoma detected at baseline colonoscopy were obtained from 17 UK hospitals between 2001 and 2010. Multivariable Cox regression models were used to estimate adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) for PCC, and, for comparison, distal CRC incidence, by adenoma characteristics.
Results: Among 18,431 patients, 152 and 105 developed PCC and distal CRC, respectively, over a median follow-up of 9.8 years. Baseline adenoma characteristics positively associated with PCC incidence included number (≥3 vs. < 3: aHR 2.10, 95% CI: 1.42-3.09), histology (tubulovillous/villous vs. tubular: aHR 1.61, 95% CI: 1.10-2.35) and location (any proximal vs. distal only: aHR 1.70, 95% CI: 1.20-2.42), for which there was borderline evidence of heterogeneity by subsite (p = 0.055). Adenoma dysplasia (high vs. low grade) was associated with distal CRC (aHR 2.42, 95% CI: 1.44-4.04), but not PCC (p-heterogeneity = 0.023).
Conclusions: Baseline adenoma number, histology and proximal location were independently associated with PCC and may be important to identify patients at higher risk for post-polypectomy PCC.
© 2022. The Author(s).
Conflict of interest statement
JK reports grants from H2020—Innovative Training Networks (ITN) grant, National Institute of Health Research (NIHR)—i4i grant, Cancer Research UK fellowship and Johnson and Johnson Educational grant, consultancy fees from Verb robotics/Ethicon, LNC therapeutics, UDX diagnostics, speaker fees from Yakult, Johnson and Johnson and shares in Cerulean health, One Welbeck day surgery and Mangetoo.com. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
