

Cardiac sympathetic innervation in Parkinson's disease versus multiple system atrophy
- PMID: 35149937
- PMCID: PMC9064856
- DOI: 10.1007/s10286-022-00853-6
Cardiac sympathetic innervation in Parkinson's disease versus multiple system atrophy
Abstract
Purpose: The aims of this study were to evaluate the diagnostic accuracy of the dual imaging method combining cardiac iodine-123-metaiodobenzylguanidine single-photon emission computed tomography combined with low-dose chest computed tomography compared to routine cardiac scintigraphy, and assess regional differences in tracer distribution and the relationships between imaging and autonomic function in Parkinson's disease and multiple system atrophy.
Methods: A prospective study including 19 Parkinson's disease and 12 multiple system atrophy patients was performed. Patients underwent clinical evaluation, iodine-123-metaiodobenzylguanidine single-photon emission computed tomography combined with chest computed tomography, planar scintigraphy, and cardiovascular autonomic function tests.
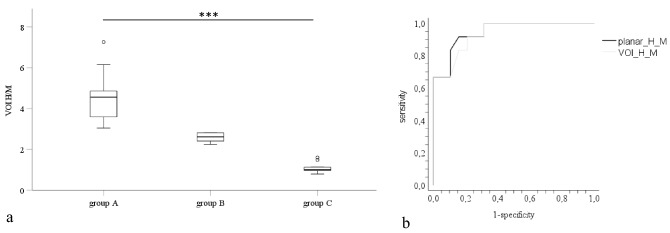
Results: Co-registration of single-photon emission computed tomography and chest computed tomography resulted in three groups with distinct patterns of tracer uptake: homogeneous, non-homogeneously reduced and absent. There was a significant difference in group allocation among patients with multiple system atrophy and Parkinson's disease (p = 0.001). Most multiple system atrophy patients showed homogeneous uptake, and the majority of Parkinson's disease patients showed absent cardiac tracer uptake. We identified a pattern of heterogeneous cardiac tracer uptake in both diseases with reductions in the apex and the lateral myocardial wall. Sympathetic dysfunction reflected by a missing blood pressure overshoot during Valsalva manoeuvre correlated with cardiac tracer distribution in Parkinson's disease patients (p < 0.001).
Conclusions: The diagnostic accuracy of the dual imaging method and routine cardiac scintigraphy were similar. Anatomical tracer allocation provided by the dual imaging method of cardiac iodine-123-metaiodobenzylguanidine single-photon emission computed tomography and chest computed tomography identified a heterogeneous subgroup of Parkinson's disease and multiple system atrophy patients with reduced cardiac tracer uptake in the apex and the lateral wall. Sympathetic dysfunction correlated with cardiac imaging in Parkinson's disease patients.
Keywords: Autonomic function; Cardiac sympathetic denervation; Multiple system atrophy; Parkinsonism; Parkinson’s disease.
© 2022. The Author(s).
Conflict of interest statement
Christine Kaindlstorfer: nothing to report. Florian Krismer: reports consultancies from the Institut de Recherches Internationales Servier, Clarion Healthcare, LLC, and grants of the MSA Coalition outside the submitted work. Eveline Donnemiller: nothing to report. Sabine Eschlböck: nothing to report. Alessandra Fanciulli: reports royalties from Springer Nature Publishing Group and Thieme Verlag, speaker fees and honoraria from International Parkinson Disease and Movement Disorders Society, IOS Press, Impact Medicom, Abbvie and Theravance Biopharma, and research grants from the Stichting ParkinsonFond, MSA Coalition, Dr Johannes Tuba Stiftung and the Österreichischer Austausch Dienst, outside of the submitted work. Cecilia Raccagni: nothing to report. Sylvia Bösch: nothing to report. Katherina Mair: nothing to report. Christoph Scherfler: nothing to report. Atbin Djamshidian: nothing to report. Christian Uprimny: nothing to report. Bernhard Metzler: nothing to report. Klaus Seppi: reports personal fees from Teva, UCB, Lundbeck, AOP Orphan Pharmaceuticals AG, Roche, Grünenthal, and Abbvie; honoraria from the International Parkinson and Movement Disorders Society; research grants from the FWF Austrian Science Fund, Michael J. Fox Foundation, and International Parkinson and Movement Disorder Society, outside the submitted work. Werner Poewe: nothing to report. Stefan Kiechl: reports support from the Austrian Research Promotion Agency FFG outside the submitted work. Irene Virgolini: nothing to report. Gregor Wenning: reports consultancy and lecture fees from AbbVie, Affiris, AstraZeneca, Biogen, Lundbeck, Merz, Novartis, Ono, Teva, and Theravance, and research grants from the FWF Austrian Science Fund, the Austrian National Bank, the US MSA-Coalition, Parkinson Fonds Austria, and International Parkinson and Movement Disorder Society outside the submitted work. The authors have no conflicts of interest to declare that are relevant to the content of this article.
Figures

Comment in
-
What new can we learn from cardiac sympathetic neuroimaging in synucleinopathies?Clin Auton Res. 2022 Apr;32(2):95-98. doi: 10.1007/s10286-022-00859-0. Epub 2022 Feb 24. Clin Auton Res. 2022. PMID: 35201527 Free PMC article. No abstract available.
References
-
- Taki J, Nakajima K, Hwang EH, Matsunari I, Komai K, Yoshita M, Sakajiri K, Tonami N. Peripheral sympathetic dysfunction in patients with Parkinson's disease without autonomic failure is heart selective and disease specific. Eur J Nucl Med. 2000;27(5):566–573. doi: 10.1007/s002590050544. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
