

Sequential lateral positioning as a new lung recruitment maneuver: an exploratory study in early mechanically ventilated Covid-19 ARDS patients
- PMID: 35150355
- PMCID: PMC8840950
- DOI: 10.1186/s13613-022-00988-9
Sequential lateral positioning as a new lung recruitment maneuver: an exploratory study in early mechanically ventilated Covid-19 ARDS patients
Abstract
Background: A sequential change in body position from supine-to-both lateral positions under constant ventilatory settings could be used as a postural recruitment maneuver in case of acute respiratory distress syndrome (ARDS), provided that sufficient positive end-expiratory pressure (PEEP) prevents derecruitment. This study aims to evaluate the feasibility and physiological effects of a sequential postural recruitment maneuver in early mechanically ventilated COVID-19 ARDS patients.
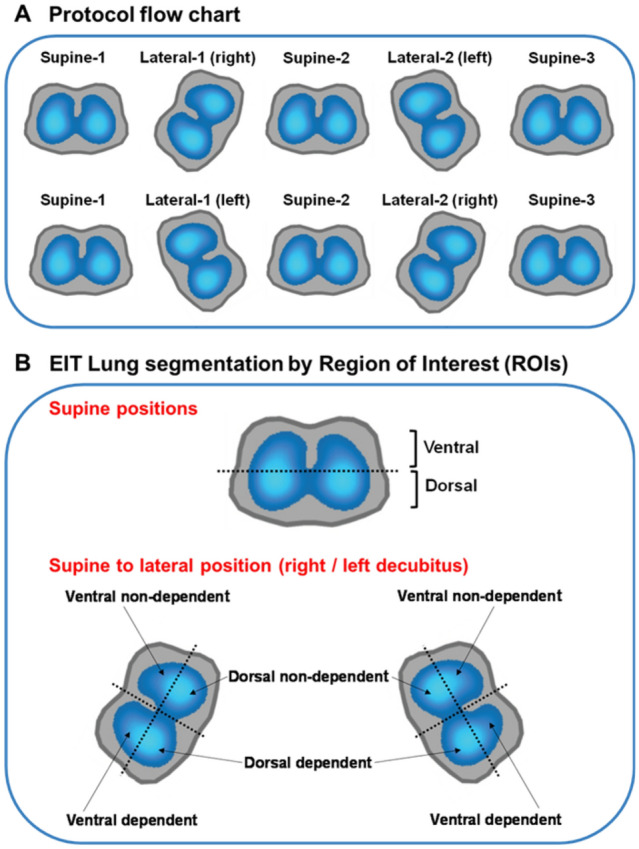
Methods: A cohort of 15 patients receiving lung-protective mechanical ventilation in volume-controlled with PEEP based on recruitability were prospectively enrolled and evaluated in five sequentially applied positions for 30 min each: Supine-baseline; Lateral-1st side; 2nd Supine; Lateral-2nd side; Supine-final. PEEP level was selected using the recruitment-to-inflation ratio (R/I ratio) based on which patients received PEEP 12 cmH2O for R/I ratio ≤ 0.5 or PEEP 15 cmH2O for R/I ratio > 0.5. At the end of each period, we measured respiratory mechanics, arterial blood gases, lung ultrasound aeration, end-expiratory lung impedance (EELI), and regional distribution of ventilation and perfusion using electric impedance tomography (EIT).
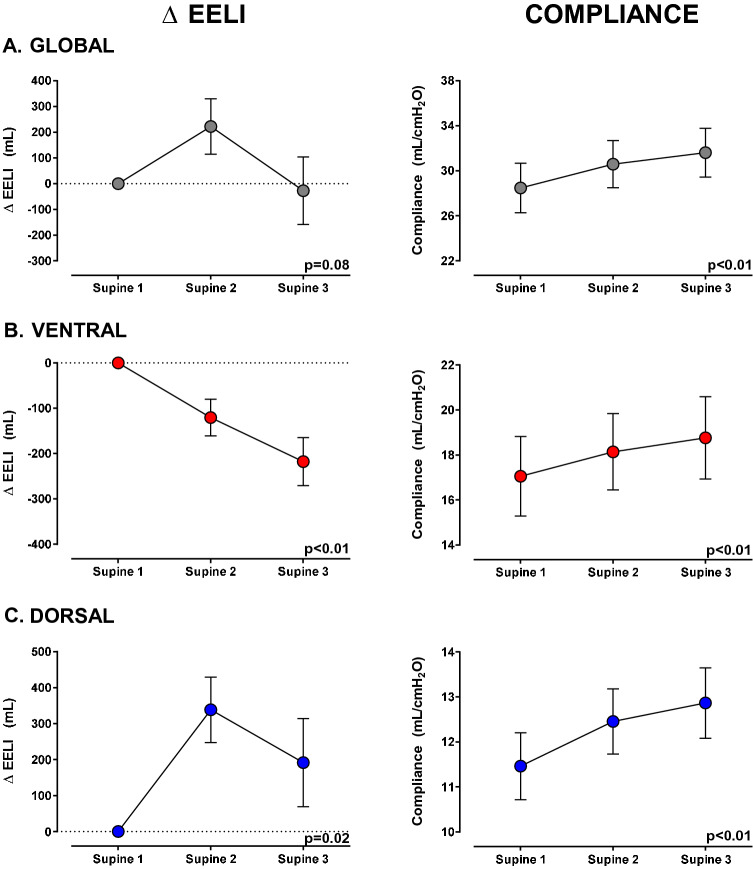
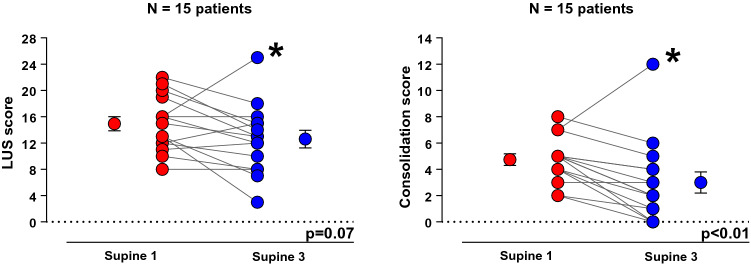
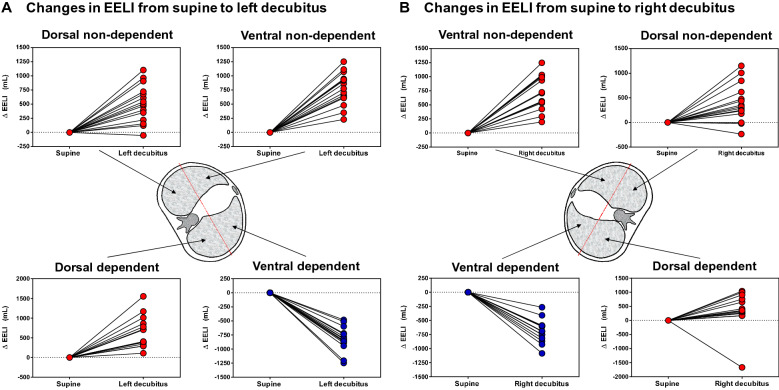
Results: Comparing supine baseline and final, respiratory compliance (29 ± 9 vs 32 ± 8 mL/cmH2O; p < 0.01) and PaO2/FIO2 ratio (138 ± 36 vs 164 ± 46 mmHg; p < 0.01) increased, while driving pressure (13 ± 2 vs 11 ± 2 cmH2O; p < 0.01) and lung ultrasound consolidation score decreased [5 (4-5) vs 2 (1-4); p < 0.01]. EELI decreased ventrally (218 ± 205 mL; p < 0.01) and increased dorsally (192 ± 475 mL; p = 0.02), while regional compliance increased in both ventral (11.5 ± 0.7 vs 12.9 ± 0.8 mL/cmH2O; p < 0.01) and dorsal regions (17.1 ± 1.8 vs 18.8 ± 1.8 mL/cmH2O; p < 0.01). Dorsal distribution of perfusion increased (64.8 ± 7.3% vs 66.3 ± 7.2%; p = 0.01).
Conclusions: Without increasing airway pressure, a sequential postural recruitment maneuver improves global and regional respiratory mechanics and gas exchange along with a redistribution of EELI from ventral to dorsal lung areas and less consolidation. Trial registration ClinicalTrials.gov, NCT04475068. Registered 17 July 2020, https://clinicaltrials.gov/ct2/show/NCT04475068.
Keywords: ARDS; COVID-19; PEEP; Postural lung recruitment.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests. LB’s laboratory has received research grants from Medtronic and Draeger and equipment from Sentec, Philps, Fisher Paykel and Air Liquide.
Figures
References
-
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195(9):1253–1263. doi: 10.1164/rccm.201703-0548ST. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
