

Casirivimab and imdevimab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial
- PMID: 35151397
- PMCID: PMC8830904
- DOI: 10.1016/S0140-6736(22)00163-5
Casirivimab and imdevimab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial
Abstract
Background: Casirivimab and imdevimab are non-competing monoclonal antibodies that bind to two different sites on the receptor binding domain of the SARS-CoV-2 spike glycoprotein, blocking viral entry into host cells. We aimed to evaluate the efficacy and safety of casirivimab and imdevimab administered in combination in patients admitted to hospital with COVID-19.
Methods: RECOVERY is a randomised, controlled, open-label platform trial comparing several possible treatments with usual care in patients admitted to hospital with COVID-19. 127 UK hospitals took part in the evaluation of casirivimab and imdevimab. Eligible participants were any patients aged at least 12 years admitted to hospital with clinically suspected or laboratory-confirmed SARS-CoV-2 infection. Participants were randomly assigned (1:1) to either usual standard of care alone or usual care plus casirivimab 4 g and imdevimab 4 g administered together in a single intravenous infusion. Investigators and data assessors were masked to analyses of the outcome data during the trial. The primary outcome was 28-day all-cause mortality assessed by intention to treat, first only in patients without detectable antibodies to SARS-CoV-2 infection at randomisation (ie, those who were seronegative) and then in the overall population. Safety was assessed in all participants who received casirivimab and imdevimab. The trial is registered with ISRCTN (50189673) and ClinicalTrials.gov (NCT04381936).
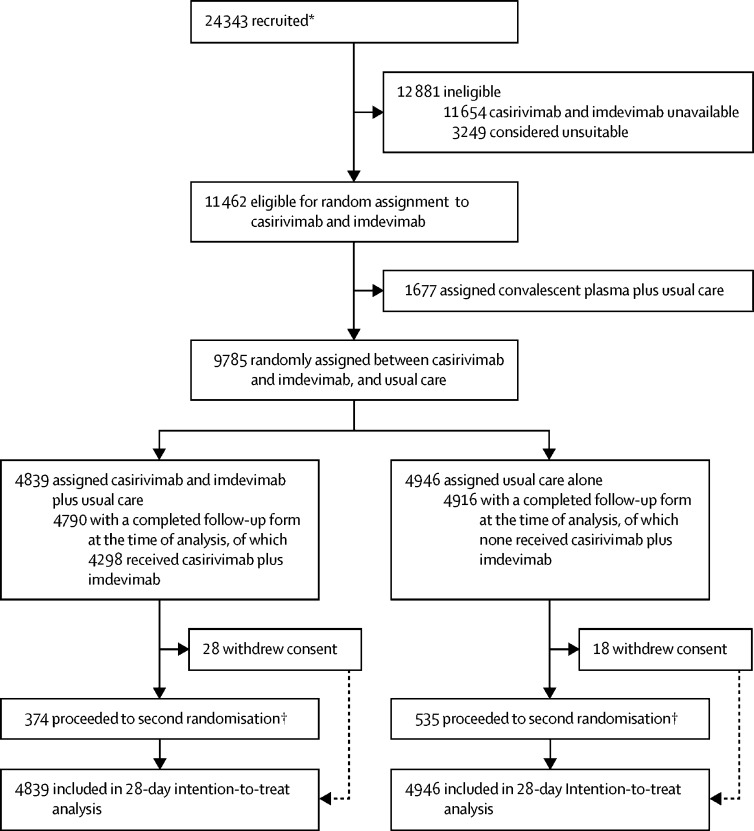
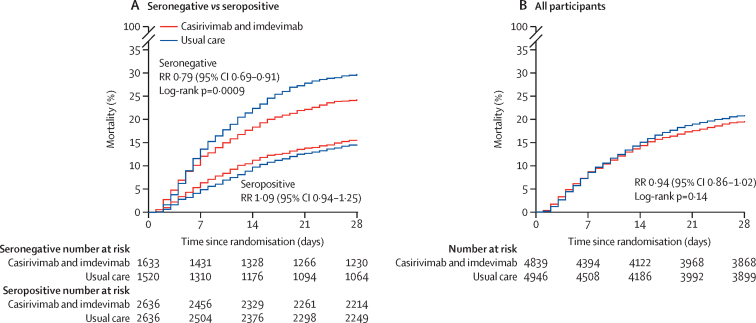
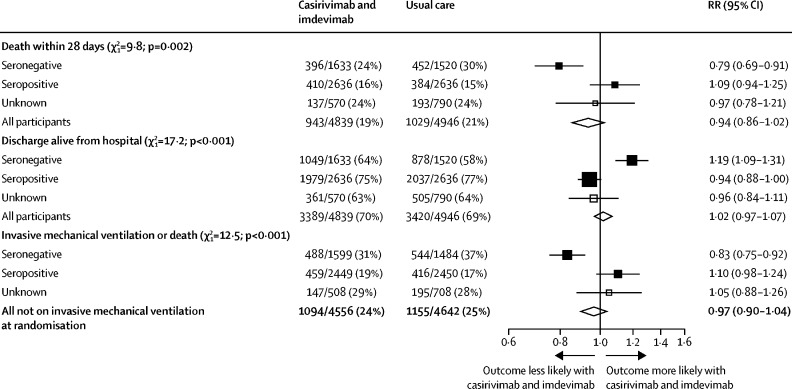
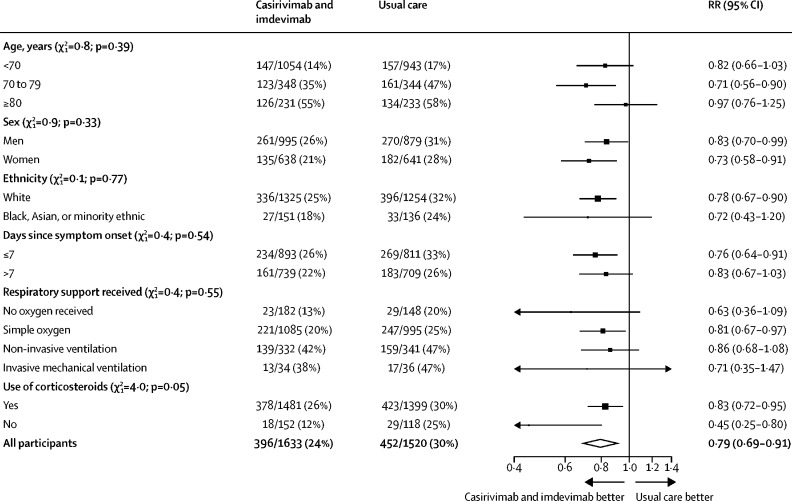
Findings: Between Sept 18, 2020, and May 22, 2021, 9785 patients enrolled in RECOVERY were eligible for casirivimab and imdevimab, of which 4839 were randomly assigned to casirivimab and imdevimab plus usual care and 4946 to usual care alone. 3153 (32%) of 9785 patients were seronegative, 5272 (54%) were seropositive, and 1360 (14%) had unknown baseline antibody status. 812 (8%) patients were known to have received at least one dose of a SARS-CoV-2 vaccine. In the primary efficacy population of seronegative patients, 396 (24%) of 1633 patients allocated to casirivimab and imdevimab versus 452 (30%) of 1520 patients allocated to usual care died within 28 days (rate ratio [RR] 0·79, 95% CI 0·69-0·91; p=0·0009). In an analysis of all randomly assigned patients (regardless of baseline antibody status), 943 (19%) of 4839 patients allocated to casirivimab and imdevimab versus 1029 (21%) of 4946 patients allocated to usual care died within 28 days (RR 0·94, 95% CI 0·86-1·02; p=0·14). The proportional effect of casirivimab and imdevimab on mortality differed significantly between seropositive and seronegative patients (p value for heterogeneity=0·002). There were no deaths attributed to the treatment, or meaningful between-group differences in the pre-specified safety outcomes of cause-specific mortality, cardiac arrhythmia, thrombosis, or major bleeding events. Serious adverse reactions reported in seven (<1%) participants were believed by the local investigator to be related to treatment with casirivimab and imdevimab.
Interpretation: In patients admitted to hospital with COVID-19, the monoclonal antibody combination of casirivimab and imdevimab reduced 28-day mortality in patients who were seronegative (and therefore had not mounted their own humoral immune response) at baseline but not in those who were seropositive at baseline.
Funding: UK Research and Innovation (Medical Research Council) and National Institute of Health Research.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests DMW is an employee of Regeneron Pharmaceuticals and holds shares or share options in the company. All other authors declare no competing interests or financial relationships relevant to the submitted work. No form of payment was given to anyone to produce the manuscript. The Nuffield Department of Population Health at the University of Oxford has a staff policy of not accepting honoraria or consultancy fees directly or indirectly from industry (see https://www.ndph.ox.ac.uk/files/about/ndph-independence-of-research-policy-jun-20.pdf).
Figures
Comment in
-
Another piece in the COVID-19 treatment puzzle.Lancet. 2022 Feb 12;399(10325):609-610. doi: 10.1016/S0140-6736(22)00154-4. Lancet. 2022. PMID: 35151380 Free PMC article. No abstract available.
References
-
- Laustsen AH. How can monoclonal antibodies be harnessed against neglected tropical diseases and other infectious diseases? Expert Opin Drug Discov. 2019;14:1103–1112. - PubMed
-
- Palivizumab, a humanized respiratory syncytial virus monoclonal antibody, reduces hospitalization from respiratory syncytial virus infection in high-risk infants. Pediatrics. 1998;102:531–537. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
