

Effect of antiretroviral therapy care interruptions on mortality in children living with HIV
- PMID: 35152225
- PMCID: PMC10002475
- DOI: 10.1097/QAD.0000000000003194
Effect of antiretroviral therapy care interruptions on mortality in children living with HIV
Erratum in
-
Effect of antiretroviral therapy care interruptions on mortality in children living with HIV: Erratum.AIDS. 2023 Apr 1;37(5):859. doi: 10.1097/01.aids.0000922280.12586.c9. AIDS. 2023. PMID: 36919793 No abstract available.
Abstract
Objective: To evaluate the characteristics and outcomes of HIV-infected children that have care interruptions, during which the child's health status and use of medication is unknown.
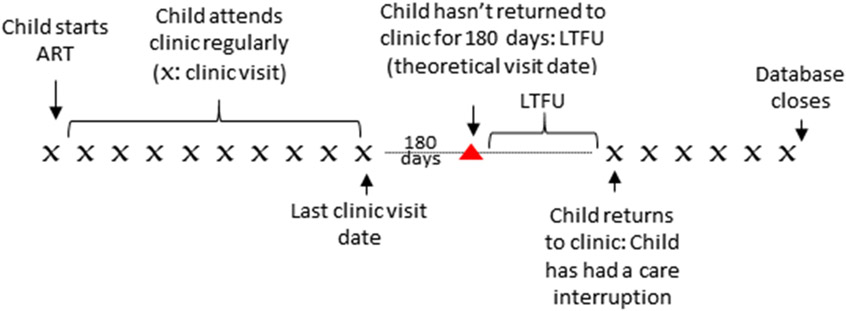
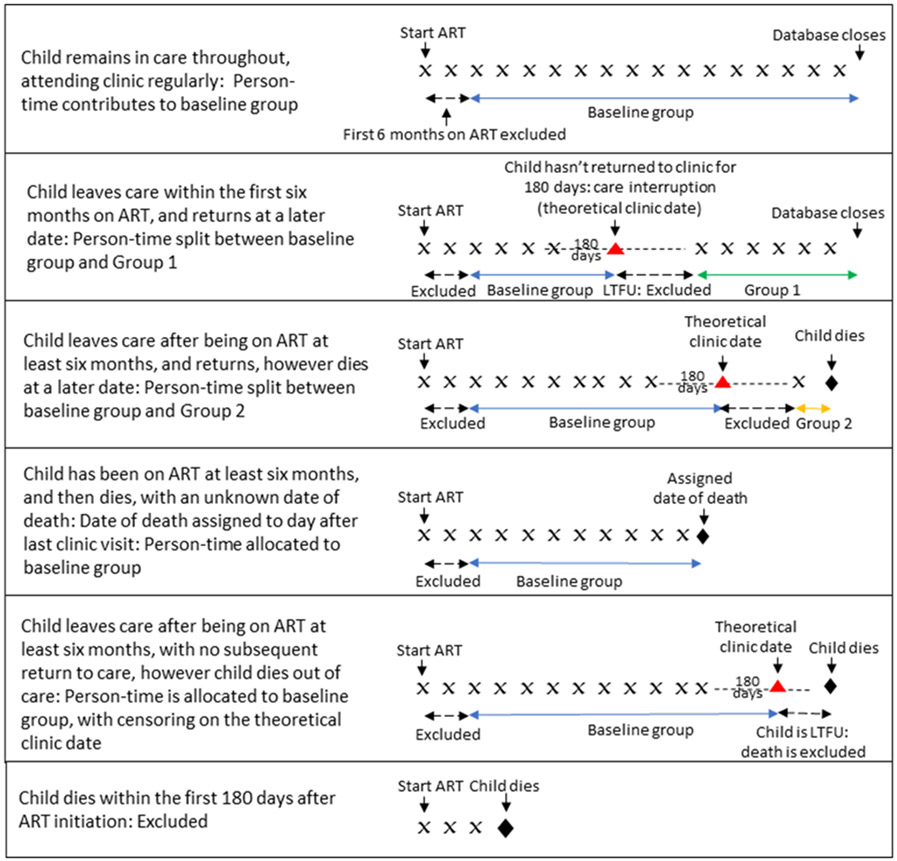
Design: We included data on children initiating ART between 2004 and 2016 at less than 16 years old at 16 International Epidemiologic Databases to Evaluate AIDS Southern Africa cohorts. Children were classified as loss to follow up (LTFU) if they had not attended clinic for more than 180 days. Children had a care interruption if they were classified as LTFU, and subsequently returned to care. Children who died within 180 days of ART start were excluded.
Methods: The main outcome was all cause mortality. Two exposed groups were considered: those with a first care interruption within the first 6 months on ART, and those with a first care interruption after 6 months on ART. Adjusted hazard ratios were determined using a Cox regression model.
Results: Among 53 674 children included, 23 437 (44%) had a care interruption, of which 10 629 (20%) had a first care interruption within 6 months on ART and 12 808 (24%) had a first care interruption after 6 months on ART. Increased mortality was associated with a care interruption within 6 months on ART [adjusted hazard ratio (AHR) = 1.52, 95% CI 1.12-2.04] but not with a care interruption after 6 months on ART (AHR = 1.05, 95% CI 0.77-1.44).
Conclusion: The findings suggest that strengthening retention of children in care in the early period after ART initiation is critical to improving paediatric ART outcomes.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest and sources of funding
There are no conflicts of interest.
Figures

References
-
- UNAIDS. UNAIDS Data 2019. Geneva; 2019.
-
- Global HIV & AIDS statistics — 2019 fact sheet. 2019.
