

Prostate cancer risk stratification improvement across multiple ancestries with new polygenic hazard score
- PMID: 35152271
- PMCID: PMC9372232
- DOI: 10.1038/s41391-022-00497-7
Prostate cancer risk stratification improvement across multiple ancestries with new polygenic hazard score
Abstract
Background: Prostate cancer risk stratification using single-nucleotide polymorphisms (SNPs) demonstrates considerable promise in men of European, Asian, and African genetic ancestries, but there is still need for increased accuracy. We evaluated whether including additional SNPs in a prostate cancer polygenic hazard score (PHS) would improve associations with clinically significant prostate cancer in multi-ancestry datasets.
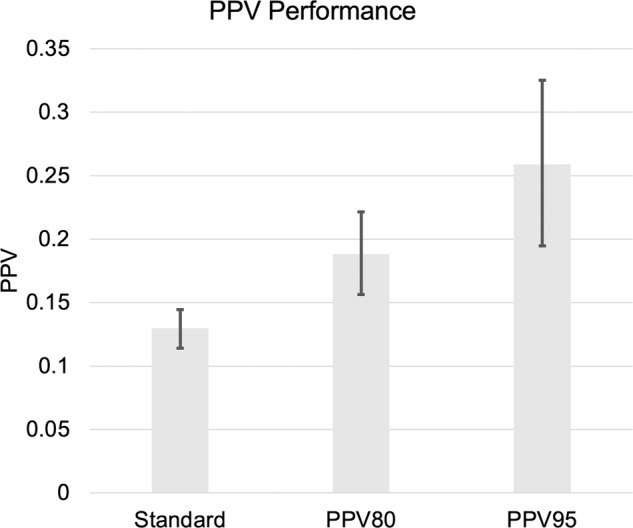
Methods: In total, 299 SNPs previously associated with prostate cancer were evaluated for inclusion in a new PHS, using a LASSO-regularized Cox proportional hazards model in a training dataset of 72,181 men from the PRACTICAL Consortium. The PHS model was evaluated in four testing datasets: African ancestry, Asian ancestry, and two of European Ancestry-the Cohort of Swedish Men (COSM) and the ProtecT study. Hazard ratios (HRs) were estimated to compare men with high versus low PHS for association with clinically significant, with any, and with fatal prostate cancer. The impact of genetic risk stratification on the positive predictive value (PPV) of PSA testing for clinically significant prostate cancer was also measured.
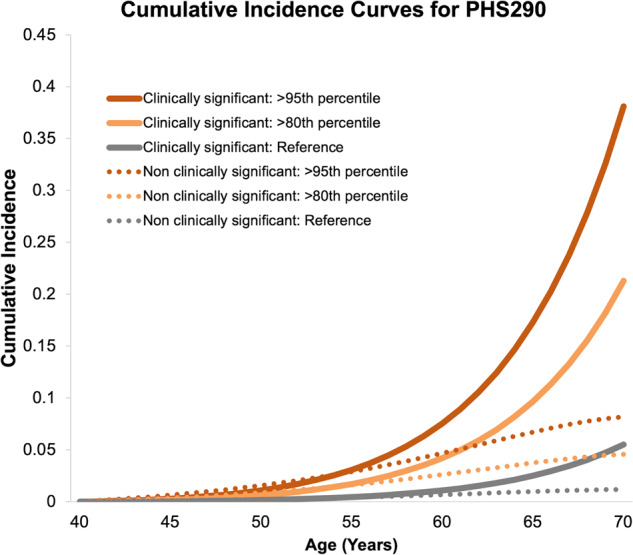
Results: The final model (PHS290) had 290 SNPs with non-zero coefficients. Comparing, for example, the highest and lowest quintiles of PHS290, the hazard ratios (HRs) for clinically significant prostate cancer were 13.73 [95% CI: 12.43-15.16] in ProtecT, 7.07 [6.58-7.60] in African ancestry, 10.31 [9.58-11.11] in Asian ancestry, and 11.18 [10.34-12.09] in COSM. Similar results were seen for association with any and fatal prostate cancer. Without PHS stratification, the PPV of PSA testing for clinically significant prostate cancer in ProtecT was 0.12 (0.11-0.14). For the top 20% and top 5% of PHS290, the PPV of PSA testing was 0.19 (0.15-0.22) and 0.26 (0.19-0.33), respectively.
Conclusions: We demonstrate better genetic risk stratification for clinically significant prostate cancer than prior versions of PHS in multi-ancestry datasets. This is promising for implementing precision-medicine approaches to prostate cancer screening decisions in diverse populations.
© 2022. The Author(s).
Conflict of interest statement
All authors declare no support from any organization for the submitted work except as follows: AMD and TMS report a past research grant from the US Department of Defense. OAA reports research grants from K.G Jebsen Stiftelsen, Research Council of Norway, and South East Norway Health Authority. Authors declare no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years except as follows, with all of these relationships outside the present study: TMS reports honoraria from Multimodal Imaging Services Corporation, Varian Medical Systems, and WebMD; he has an equity interest in CorTechs Labs and also serves on its Scientific Advisory Board. These companies might potentially benefit from the research results. The terms of this arrangement have been reviewed and approved by the University of California San Diego in accordance with its conflict-of-interest policies. OAA reports speaker honoraria from Lundbeck. Authors declare no other relationships or activities that could appear to have influenced the submitted work except as follows: OAA has a patent application # U. S. 20150356243 pending; AMD also applied for this patent application and assigned it to UC San Diego. AMD has additional disclosures outside the present work: founder, equity holder, and advisory board member for CorTechs Labs, Inc.; founder and equity holder in HealthLytix, Inc., advisory board member of Human Longevity, Inc.; recipient of nonfinancial research support from General Electric Healthcare. OAA is a consultant for HealthLytix, Inc. Additional acknowledgments for the PRACTICAL consortium and contributing studies are described in the Supplementary Information.
Figures
References
-
- Callender T, Emberton M, Morris S, Pharoah PDP, Pashayan N. Benefit, Harm, and Cost-effectiveness Associated with Magnetic Resonance Imaging before Biopsy in Age-based and Risk-stratified Screening for Prostate Cancer. JAMA Network Open. 2021;4:2037657. doi: 10.1001/jamanetworkopen.2020.37657. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
