

Effectiveness of golimumab in patients with ulcerative colitis: results of a real-life study in Switzerland
- PMID: 35154389
- PMCID: PMC8832575
- DOI: 10.1177/17562848221074188
Effectiveness of golimumab in patients with ulcerative colitis: results of a real-life study in Switzerland
Abstract
Background: Tumor necrosis factor (TNF) inhibitors have improved treatment of ulcerative colitis (UC), but loss of response remains a frequent problem. The anti-TNF agent, golimumab, was approved in Switzerland for the treatment of UC in 2014. This study aims to summarize the experience of golimumab in a real-world setting in Switzerland.
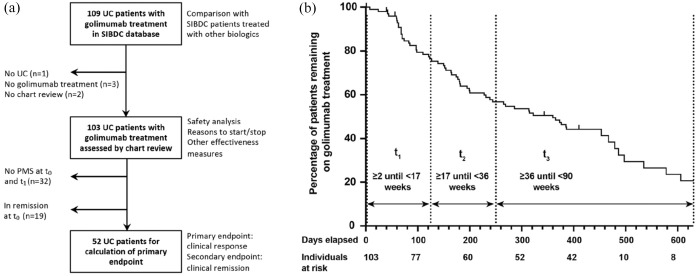
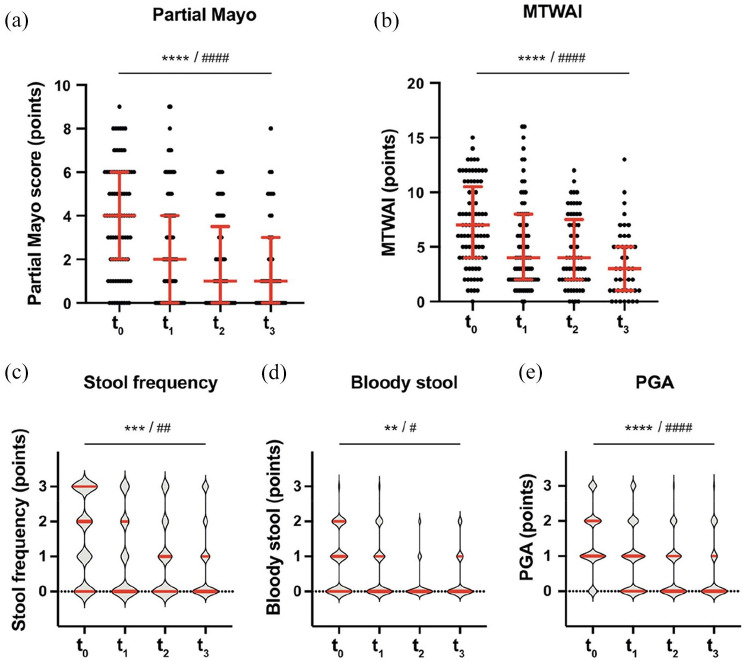
Methods: We analyzed real-world data from 1769 UC patients from the Swiss Inflammatory Bowel Disease Cohort (SIBDC) study and performed a chart review of golimumab-treated patients. We extracted the partial Mayo score at t0 (baseline), t1 (2-16 weeks), t2 (17-35 weeks), and t3 (36-89 weeks). The primary endpoint was clinical response at t1, defined as marked improvement in partial Mayo score and objective parameters. Clinical remission was defined as resolution of symptoms and normalization of objective parameters.
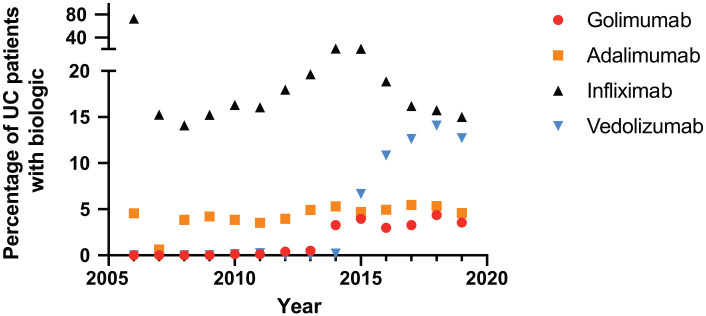
Results: Our chart review included 103 UC patients with golimumab treatment (5.8% of all SIBDC UC patients); only 16 (15.5%) were anti-TNF naïve. Sixty-three patients remained on golimumab (61.2%) after 180 days, 51 (44.7%) after 365 days, and 34 (33%) after 630 days after the start of treatment. Upon golimumab treatment, the partial Mayo score decreased from 4 [interquartile range (IQR): 2-6] at t0 to 2 (IQR: 0-4) at t1, 1 (IQR: 0-3.5) at t2, and 1 (IQR: 0-3) at t3 (p < 0.001 for all comparisons with t0). The primary endpoint, clinical response at t1, could be evaluated in 52 patients and was met in 15 individuals (28.8%). Clinical remission at t1 was observed in 8 out of 52 patients (15.4%). Golimumab was generally well tolerated, one patient developed meningitis. The most frequent reasons to stop treatment were primary and secondary non-response.
Conclusion: Golimumab was used in 5.8% of Swiss UC patients, mainly in biologic-experienced individuals. Golimumab treatment was associated with a sustained reduction of symptoms and clinical response in approximately 30% of patients.[ClinicalTrials.gov identifier: NCT00488631].
Keywords: TNF inhibitor; golimumab; inflammatory bowel disease; ulcerative colitis.
© The Author(s), 2022.
Conflict of interest statement
Conflict of interest statement: The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KP has nothing to disclose. NK has nothing to disclose. SBUJ has nothing to disclose. JBR has nothing to disclose. LB reports fees for consulting/advisory board from Abbvie, MSD, Vifor, Falk, Esocap, Calypso, Ferring, Pfizer, Shire, Takeda, Janssen, and Ewopharma. TG has consulting contracts with Sanofi-Regeneron and Falk Pharma GmbH, received travel grants from Falk Pharma GmbH and Vifor, and an unrestricted research grant from Novartis. PS has consulted to Pfizer, Takeda, Abbvie, and Janssen-Cilag and received travel support from Falk and UCB. SRV has received consulting fees, speakers honorary, and unrestricted research grants from Abbott, Alfasigma, Amgen, Arenapharm, Falk Pharma GmbH, Ferring Pharmaceuticals, Gilead, iQuone, Janssen, MSD, Permamed, Pfizer Inc, Sanofi-Aventis, Takeda, Tillotts, UCB, and Vifor. PJ has received a research grant from Vifor unrelated to this work. EB received consultant and/or speaker fees from Abbvie, Janssen, MSD, Norgine, Pfizer, Sandoz, Takeda, and Vifor. DZ has nothing to disclose. MHM has received consultant fees from Vifor, Abbvie, UCB, MSD, Lilly, Janssen, and Takeda. He also received grants from UCB, Abbvie, Vifor, MSD, Takeda. He received speaker fess from Vifor, Janssen, Abbvie, MSD, Pfizer, UCB, and Takeda. MCS has received consultant and/or speaker fees from Abbvie, Ferring, MSD, Janssen, Pfizer, Takeda, UCB. SB has consulted to Abbvie, Celgene, Ferring, Gilead, Janssen, MSD, Pfizer, Roche, UCB, and Takeda, Vifor; SB has received speaker’s honoraria from Abbvie, FALK, Ferring, MSD, Takeda, UCB, and Vifor; SB has received an educational grant from Takeda. GR has consulted to Abbvie, Augurix, BMS, Boehringer, Calypso, Celgene, FALK, Ferring, Fisher, Genentech, Gilead, Janssen, MSD, Novartis, Pfizer, Phadia, Roche, UCB, Takeda, Tillots, Vifor, Vital Solutions, and Zeller; GR has received speaker’s honoraria from Astra Zeneca, Abbvie, FALK, Janssen, MSD, Pfizer, Phadia, Takeda, Tillots, UCB, Vifor, and Zeller; GR has received educational grants and research grants from Abbvie, Ardeypharm, Augurix, Calypso, FALK, Flamentera, MSD, Novartis, Pfizer, Roche, Takeda, Tillots, UCB, and Zeller. BM has received a research grant from MSD for this work. BM has served at an advisory board for Gilead and Novigenix. He has received speaking fees from Vifor, MSD, and Takeda and traveling fees from Vifor, Novartis, Gilead, and Takeda.
Figures
References
-
- Singh S, Fumery M, Sandborn WJ, et al.. Systematic review with network meta-analysis: first- and second-line pharmacotherapy for moderate-severe ulcerative colitis. Aliment Pharmacol Ther 2018; 47: 162–175. - PubMed
-
- Misselwitz B, Juillerat P, Sulz MC, et al.. Emerging treatment options in inflammatory bowel disease: Janus kinases, stem cells, and more. Digestion 2020; 101(Suppl. 1): 69–82. - PubMed
-
- Ben-Horin S, Kopylov U, Chowers Y. Optimizing anti-TNF treatments in inflammatory bowel disease. Autoimmun Rev 2014; 13: 24–30. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
