

Inflammatory marker trajectories associated with frailty and ageing in a 20-year longitudinal study
- PMID: 35154709
- PMCID: PMC8826353
- DOI: 10.1002/cti2.1374
Inflammatory marker trajectories associated with frailty and ageing in a 20-year longitudinal study
Abstract
Objective: The aim of this exploratory study was to investigate the development of low-grade inflammation during ageing and its relationship with frailty.
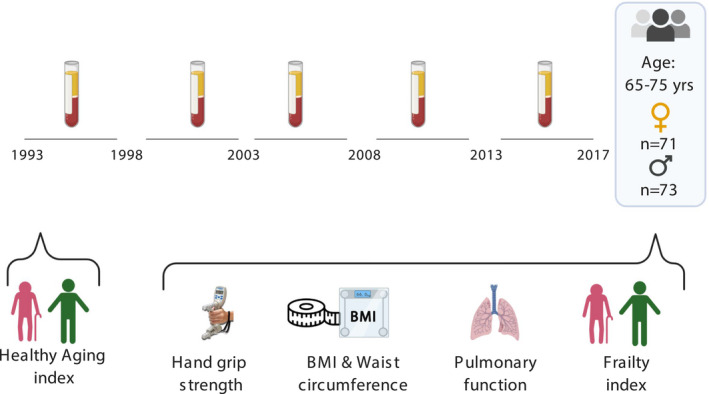
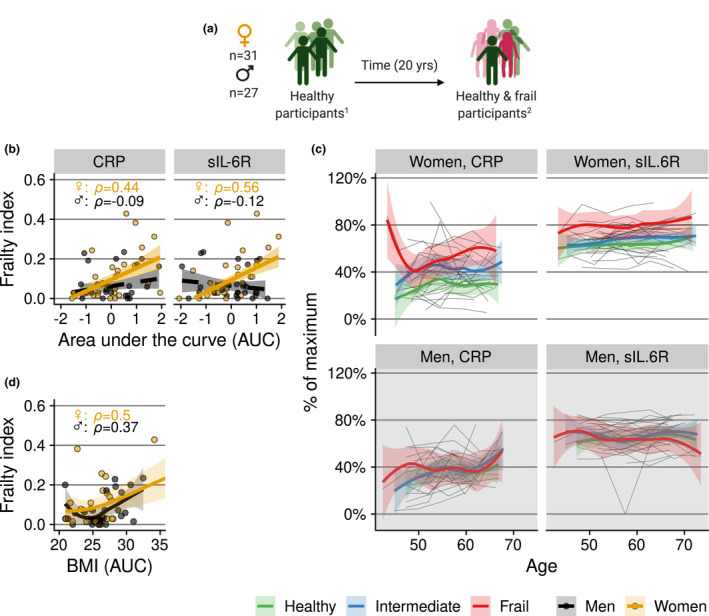
Methods: The trajectories of 18 inflammatory markers measured in blood samples, collected at 5-year intervals over a period of 20 years from 144 individuals aged 65-75 years at the study endpoint, were related to the degree of frailty later in life.
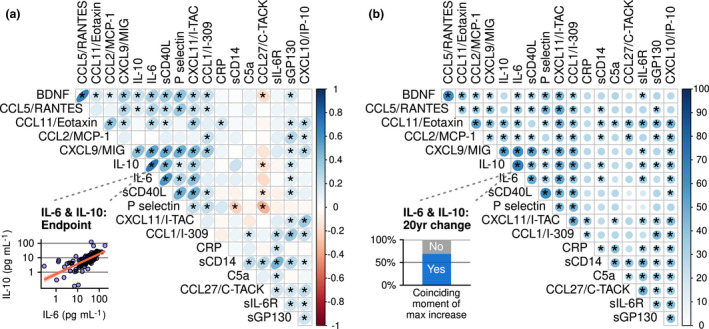
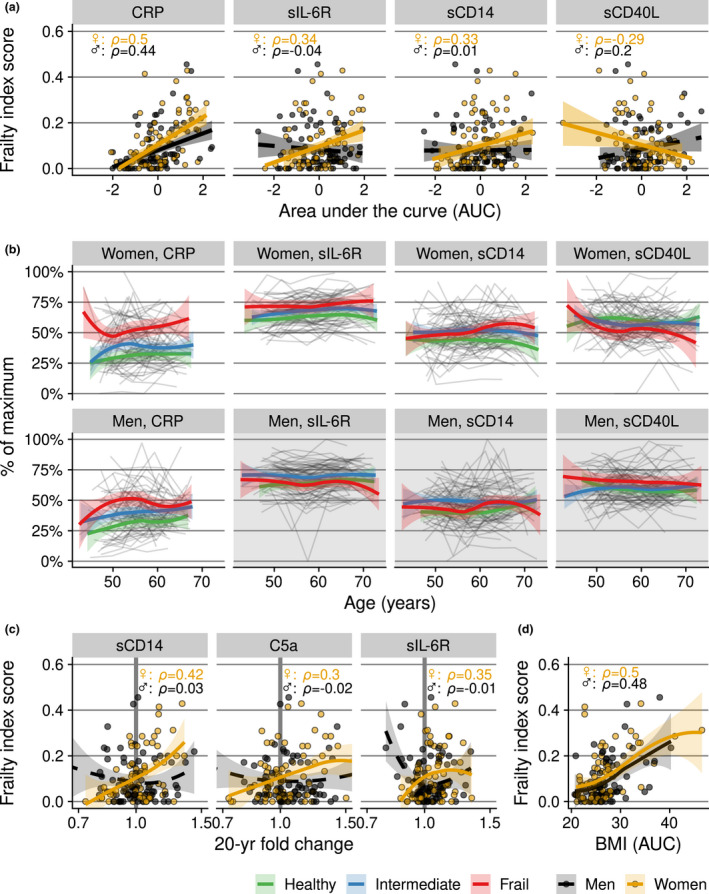
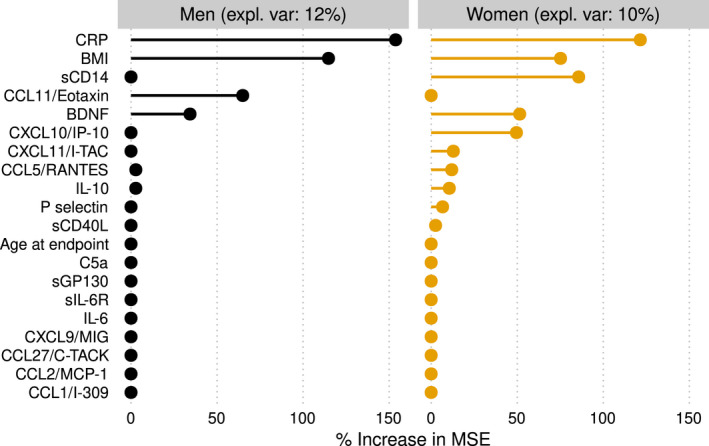
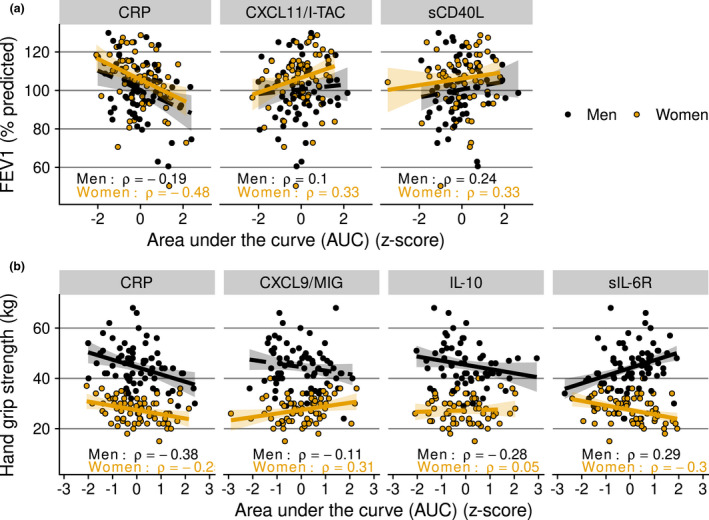
Results: IFN-γ-related markers and platelet activation markers were found to change in synchrony. Chronically elevated levels of IL-6 pathway markers, such as CRP and sIL-6R, were associated with more frailty, poorer lung function and reduced physical strength. Being overweight was a possible driver of these associations. More and stronger associations were detected in women, such as a relation between increasing sCD14 levels and frailty, indicating a possible role for monocyte overactivation. Multivariate prediction of frailty confirmed the main results, but predictive accuracy was low.
Conclusion: In summary, we documented temporal changes in and between inflammatory markers in an ageing population over a period of 20 years, and related these to clinically relevant health outcomes.
Keywords: chemokines; chronic low‐grade inflammation; cytokines; frailty; healthy ageing; longitudinal study.
© 2022 The Authors. Clinical & Translational Immunology published by John Wiley & Sons Australia, Ltd on behalf of Australian and New Zealand Society for Immunology, Inc.
Conflict of interest statement
The authors declare no conflict of interest. Author Contributions Leonard Daniël Samson: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Software; Validation; Visualization; Writing – original draft; Writing – review & editing. Anne‐Marie Buisman: Conceptualization; Funding acquisition; Supervision; Writing – review & editing. José A Ferreira: Formal analysis; Methodology; Writing – review & editing. H Susan J Picavet: Resources; Writing – review & editing. W M Monique Verschuren: Resources; Supervision; Writing – review & editing. Annemieke M H Boots: Conceptualization; Project administration; Supervision; Writing – review & editing. Peter Engelfriet: Conceptualization; Funding acquisition; Investigation; Methodology; Supervision; Writing – review & editing.
Figures
References
-
- United Nations . World Population Ageing 2015. UN; 2017. https://www.un‐ilibrary.org/population‐and‐demography/world‐population‐a... (accessed 3 July 2020).
-
- Franceschi C, Garagnani P, Vitale G, Capri M, Salvioli S. Inflammaging and ‘Garb‐aging’. Trends in Endocr Metab 2017; 28: 199–212. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous