

Rotator Cuff Repair Using Coracoacromial Ligament Autograft for Supraspinatus Footprint Augmentation
- PMID: 35155113
- PMCID: PMC8821721
- DOI: 10.1016/j.eats.2021.10.011
Rotator Cuff Repair Using Coracoacromial Ligament Autograft for Supraspinatus Footprint Augmentation
Abstract
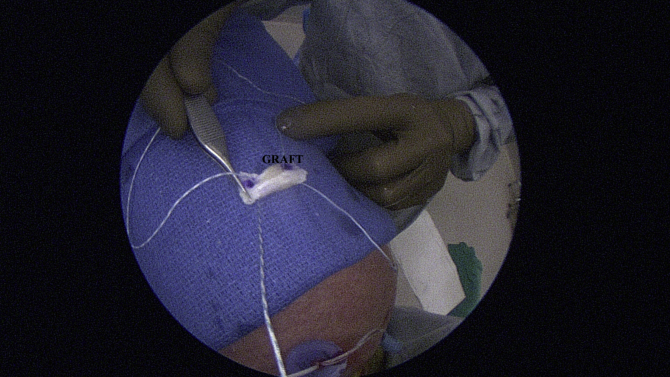
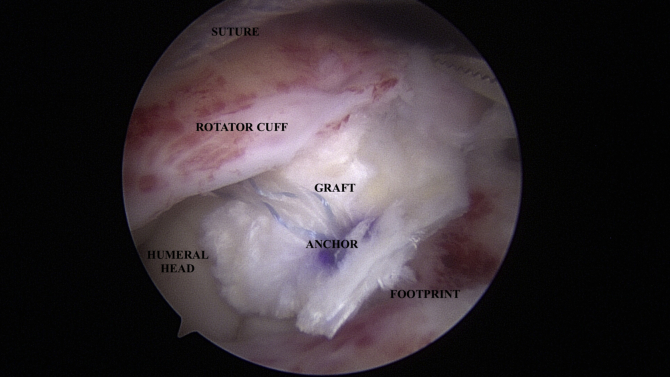
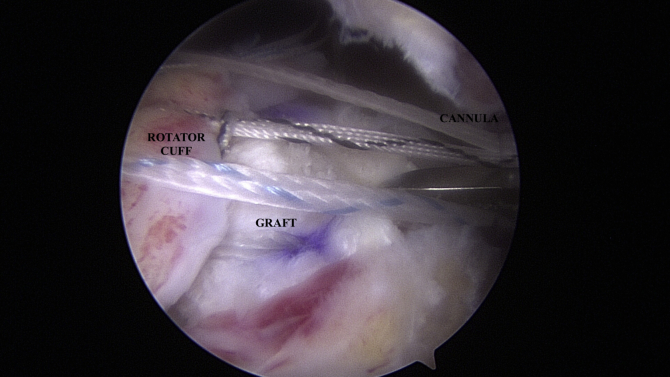
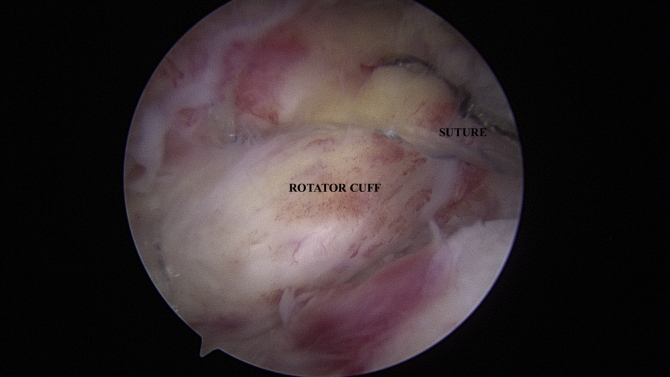
Failure of rotator cuff repair can be a disastrous clinical outcome. Although failure is a multifactorial issue, recent interest has piqued in understanding the biology of the insertional components of the supraspinatus and infraspinatus at the footprint. When the torn tendon is of poor quality, especially if it is diminutive or thin, rotator cuff repair augmentation should be considered to aid in long-term healing. Various allograft options have been described in the past, and more recently, xenografts and synthetics have become more commonly used. The use of autografts in the treatment of insertional footprint deficiency has great potential; however, few grafts have been described. This study describes the surgical technique for footprint augmentation in arthroscopic supraspinatus repair using harvested autologous coracoacromial ligament tissue.
© 2021 The Authors.
Figures

Similar articles
-
Combining fascia lata autograft bridging repair with artificial ligament internal brace reinforcement : a novel healing-improvement technique for irreparable massive rotator cuff tears.Bone Joint J. 2021 Oct;103-B(10):1619-1626. doi: 10.1302/0301-620X.103B10.BJJ-2020-2546.R2. Bone Joint J. 2021. PMID: 34587809
-
Intratendinous Strain Variations of the Supraspinatus Tendon Depending on Repair Technique: A Biomechanical Analysis Regarding the Cause of Medial Cuff Failure.Am J Sports Med. 2021 Jun;49(7):1847-1853. doi: 10.1177/03635465211006138. Epub 2021 Apr 19. Am J Sports Med. 2021. PMID: 33872064
-
Healing and Functional Results of Dermal Allograft Augmentation of Complex and Revision Rotator Cuff Repairs.Am J Sports Med. 2021 Jul;49(8):2042-2047. doi: 10.1177/03635465211015194. Epub 2021 May 20. Am J Sports Med. 2021. PMID: 34015245
-
Outcomes of rotator cuff surgery: what does the evidence tell us?Clin Sports Med. 2012 Oct;31(4):665-74. doi: 10.1016/j.csm.2012.07.004. Clin Sports Med. 2012. PMID: 23040552 Review.
-
Augmentation of Rotator Cuff Repair With Soft Tissue Scaffolds.Orthop J Sports Med. 2015 Jun 10;3(6):2325967115587495. doi: 10.1177/2325967115587495. eCollection 2015 Jun. Orthop J Sports Med. 2015. PMID: 26665095 Free PMC article. Review.
References
-
- Mirzayan R., Weber A.E., Petrigliano F.A., Chahla J. Rationale for biologic augmentation of rotator cuff repairs. J Am Acad Orthop Surg. 2019;27:468–478. - PubMed
-
- Bailey J.R., Kim C., Alentorn-Geli E., et al. Rotator cuff matrix augmentation and interposition: A systematic review and meta-analysis. Am J Sports Med. 2019;47:1496–1506. - PubMed
-
- Le Hanneur M., Delgrande D., Lafosse T., Werthel J.D., Hardy P., Elhassan B. Triple-bundle anatomical reconstruction using the coracoacromial ligament and the short head of biceps tendon to stabilize chronic acromioclavicular joint dislocations: A cadaver feasibility study. Orthop Traumatol Surg Res. 2018;104:27–32. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
