

Development and Validation of a CT-Based Radiomics Nomogram for Predicting Postoperative Progression-Free Survival in Stage I-III Renal Cell Carcinoma
- PMID: 35155180
- PMCID: PMC8830916
- DOI: 10.3389/fonc.2021.742547
Development and Validation of a CT-Based Radiomics Nomogram for Predicting Postoperative Progression-Free Survival in Stage I-III Renal Cell Carcinoma
Abstract
Background: Many patients experience recurrence of renal cell carcinoma (RCC) after radical and partial nephrectomy. Radiomics nomogram is a newly used noninvasive tool that could predict tumor phenotypes.
Objective: To investigate Radiomics Features (RFs) associated with progression-free survival (PFS) of RCC, assessing its incremental value over clinical factors, and to develop a visual nomogram in order to provide reference for individualized treatment.
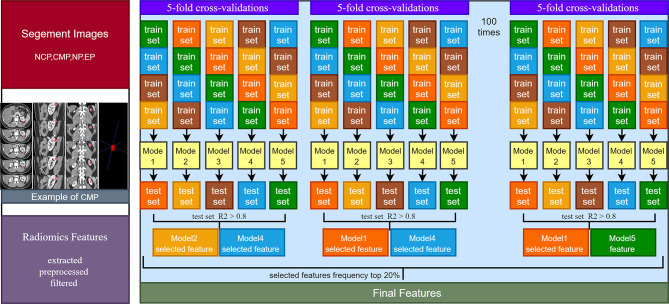
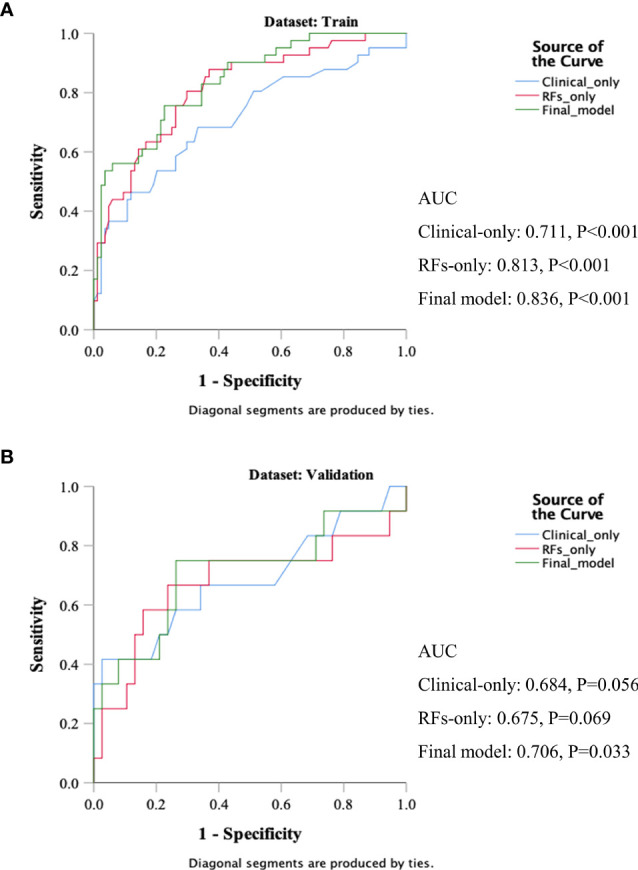
Methods: The RFs and clinicopathological data of 175 patients (125 in the training set and 50 in the validation set) with clear cell RCC (ccRCC) were retrospectively analyzed. In the training set, RFs were extracted from multiphase enhanced CT tumor volume and selected using the stability LASSO feature selection algorithm. A radiomics nomogram final model was developed that incorporated the RFs weighted sum and selected clinical predictors based on the multivariate Cox proportional hazard regression. The performances of a clinical variables-only model, RFs-only model, and the final model were compared by receiver operator characteristic (ROC) analysis and DeLong test. Nomogram performance was determined and validated with respect to its discrimination, calibration, reclassification, and clinical usefulness.
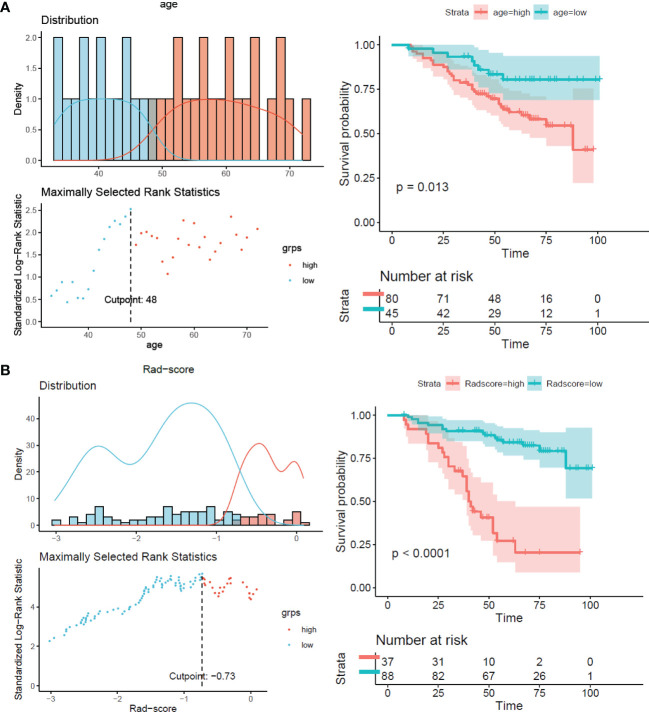
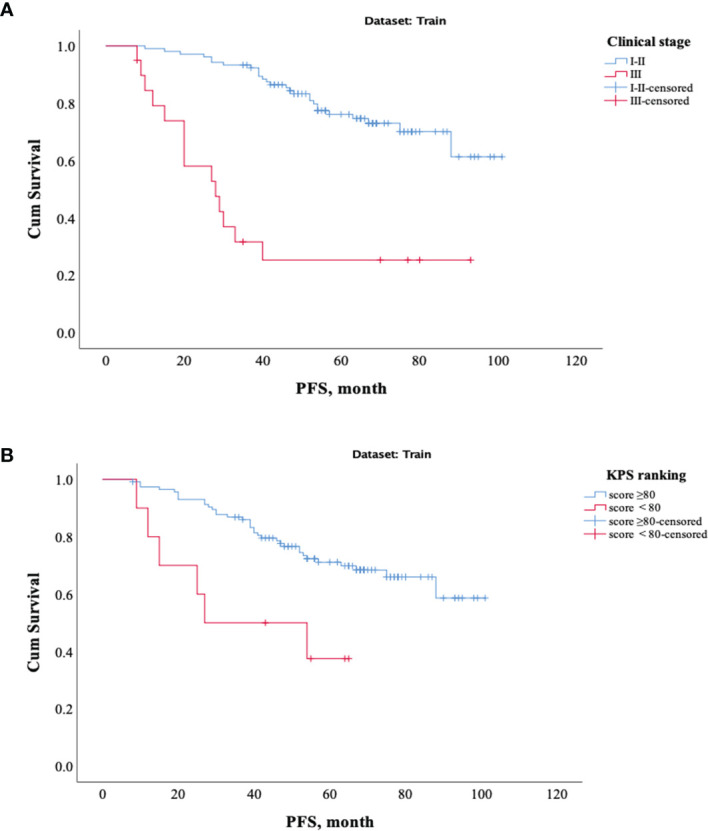
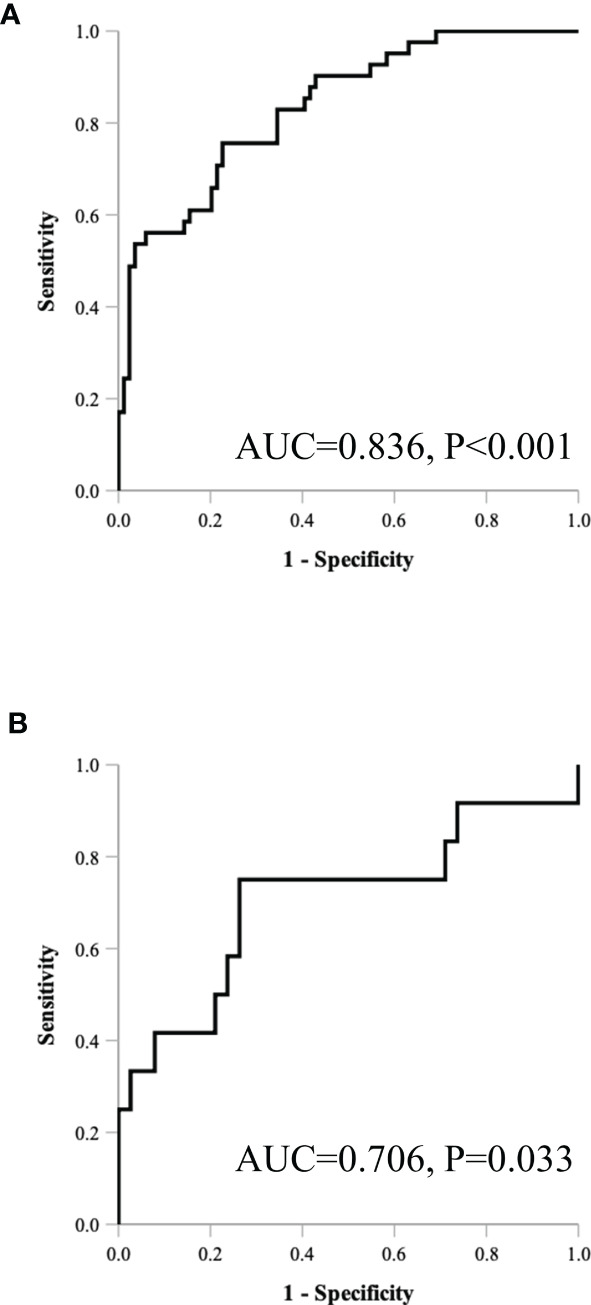
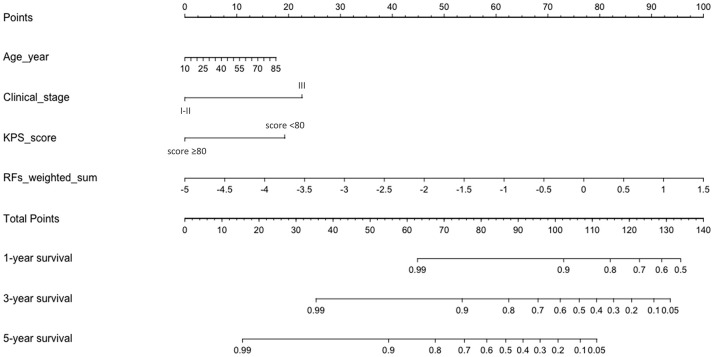
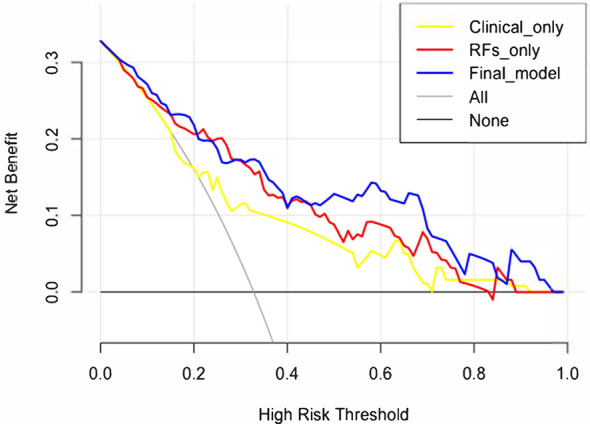
Results: The radiomics nomogram included age, clinical stage, KPS score, and RFs weighted sum, which consisted of 6 selected RFs. The final model showed good discrimination, with a C-index of 0.836 and 0.706 in training and validation, and good calibration. In the training set, the C-index of the final model was significantly larger than the clinical-only model (DeLong test, p = 0.008). From the clinical variables-only model to the final model, the reclassification of net reclassification improvement was 18.03%, and the integrated discrimination improvement was 19.08%. Decision curve analysis demonstrated the clinical usefulness of the radiomics nomogram.
Conclusion: The CT-based RF is an improvement factor for clinical variables-only model. The radiomics nomogram provides individualized risk assessment of postoperative PFS for patients with RCC.
Keywords: CT; Radiomics; artificial intelligence; predict model; progression-free survival (PFS); renal cell carcinoma (RCC).
Copyright © 2022 Zhang, Yin, Chen, Yang, Qi, Cui, Yang and Wen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Predicting postoperative recurrence of stage Ⅰ-Ⅲ renal clear cell carcinoma based on preoperative CT radiomics feature nomogram].Nan Fang Yi Ke Da Xue Xue Bao. 2021 Aug 31;41(9):1358-1365. doi: 10.12122/j.issn.1673-4254.2021.09.10. Nan Fang Yi Ke Da Xue Xue Bao. 2021. PMID: 34658350 Free PMC article. Chinese.
-
Development and validation of a CT-based nomogram for preoperative prediction of clear cell renal cell carcinoma grades.Eur Radiol. 2021 Aug;31(8):6078-6086. doi: 10.1007/s00330-020-07667-y. Epub 2021 Jan 29. Eur Radiol. 2021. PMID: 33515086
-
A Radiomics Signature-Based Nomogram to Predict the Progression-Free Survival of Patients With Hepatocellular Carcinoma After Transcatheter Arterial Chemoembolization Plus Radiofrequency Ablation.Front Mol Biosci. 2021 Aug 31;8:662366. doi: 10.3389/fmolb.2021.662366. eCollection 2021. Front Mol Biosci. 2021. PMID: 34532340 Free PMC article.
-
A CT-based radiomics nomogram for predicting the progression-free survival in small cell lung cancer: a multicenter cohort study.Radiol Med. 2023 Nov;128(11):1386-1397. doi: 10.1007/s11547-023-01702-w. Epub 2023 Aug 19. Radiol Med. 2023. PMID: 37597124
-
A CT-based deep learning radiomics nomogram for predicting the response to neoadjuvant chemotherapy in patients with locally advanced gastric cancer: A multicenter cohort study.EClinicalMedicine. 2022 Mar 21;46:101348. doi: 10.1016/j.eclinm.2022.101348. eCollection 2022 Apr. EClinicalMedicine. 2022. PMID: 35340629 Free PMC article.
Cited by
-
Intra- and Peritumoral CT-Based Radiomics for Assessing Pathologic T-Staging in Clear Cell Renal Cell Carcinoma: A Multicenter Study.Ann Surg Oncol. 2025 Jun;32(6):4550-4561. doi: 10.1245/s10434-025-17111-4. Epub 2025 Mar 19. Ann Surg Oncol. 2025. PMID: 40106107
-
Prediction of clear cell renal cell carcinoma ≤ 4cm: visual assessment of ultrasound characteristics versus ultrasonographic radiomics analysis.Front Oncol. 2024 Jul 23;14:1298710. doi: 10.3389/fonc.2024.1298710. eCollection 2024. Front Oncol. 2024. PMID: 39114306 Free PMC article.
-
Radiomics vs radiologist in bladder and renal cancer. Results from a systematic review.Cent European J Urol. 2023;76(1):12-19. doi: 10.5173/ceju.2023.252. Epub 2023 Jan 21. Cent European J Urol. 2023. PMID: 37064257 Free PMC article. Review.
-
The influence of manual segmentation strategies and different phases selection on machine learning-based computed tomography in renal tumors: a systematic review and meta-analysis.Radiol Med. 2024 Jul;129(7):1025-1037. doi: 10.1007/s11547-024-01825-8. Epub 2024 May 13. Radiol Med. 2024. PMID: 38740709
-
Oral contrast-enhanced ultrasonographic features and radiomics analysis to predict NIH risk stratification for gastrointestinal stromal tumors.Front Oncol. 2025 Jul 3;15:1590432. doi: 10.3389/fonc.2025.1590432. eCollection 2025. Front Oncol. 2025. PMID: 40678063 Free PMC article.
References
-
- Capitanio U, Cloutier V, Zini L, Isbarn H, Jeldres C, Shariat SF, et al. . A Critical Assessment of the Prognostic Value of Clear Cell, Papillary and Chromophobe Histological Subtypes in Renal Cell Carcinoma: A Population-Based Study. Bju Int (2009) 103(11):1496–500. doi: 10.1111/j.1464-410X.2008.08259.x - DOI - PubMed
LinkOut - more resources
Full Text Sources