

Computer-Assisted Dental Implant Placement Following Free Flap Reconstruction: Virtual Planning, CAD/CAM Templates, Dynamic Navigation and Augmented Reality
- PMID: 35155183
- PMCID: PMC8833256
- DOI: 10.3389/fonc.2021.754943
Computer-Assisted Dental Implant Placement Following Free Flap Reconstruction: Virtual Planning, CAD/CAM Templates, Dynamic Navigation and Augmented Reality
Abstract
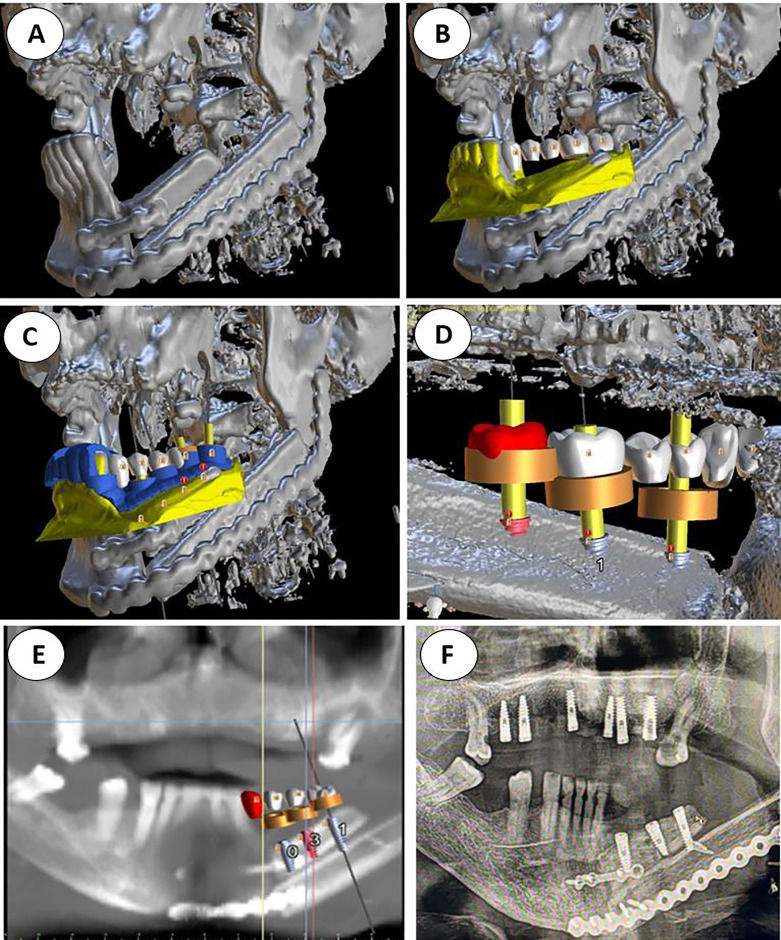
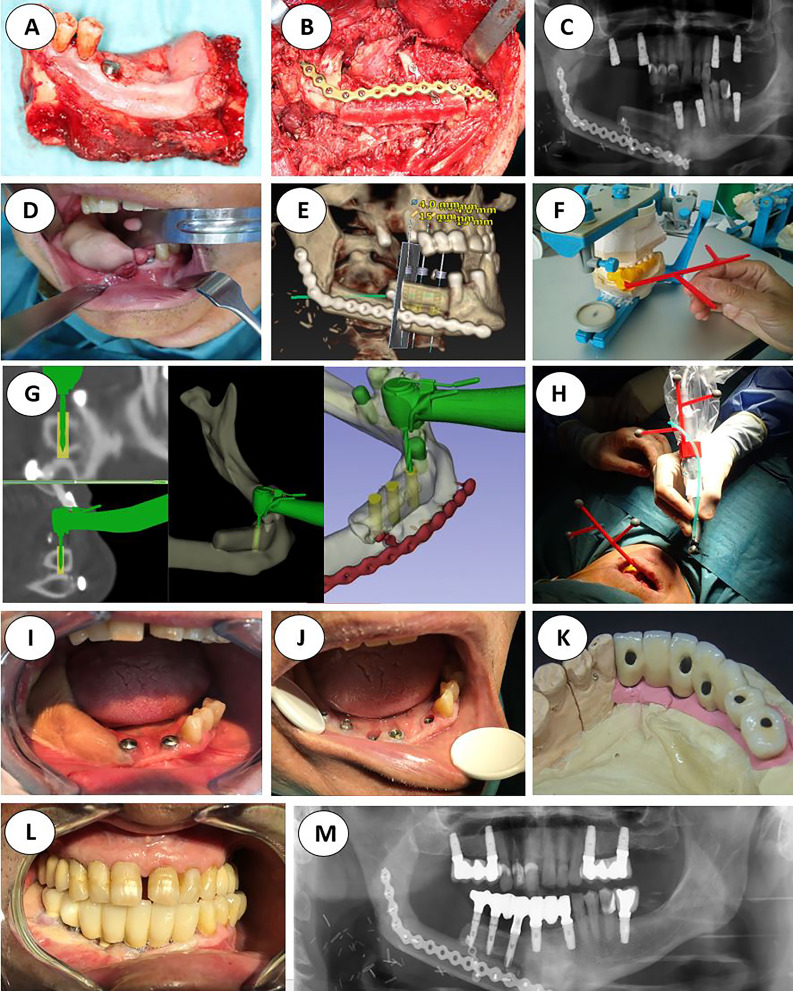
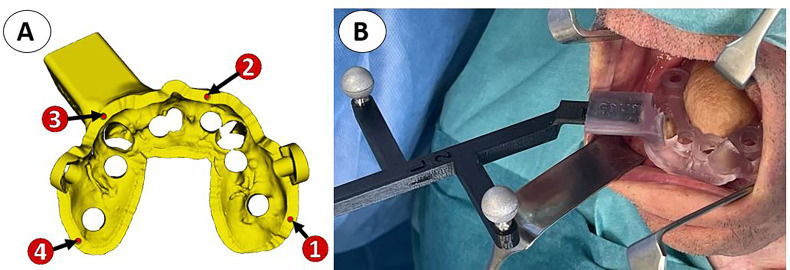
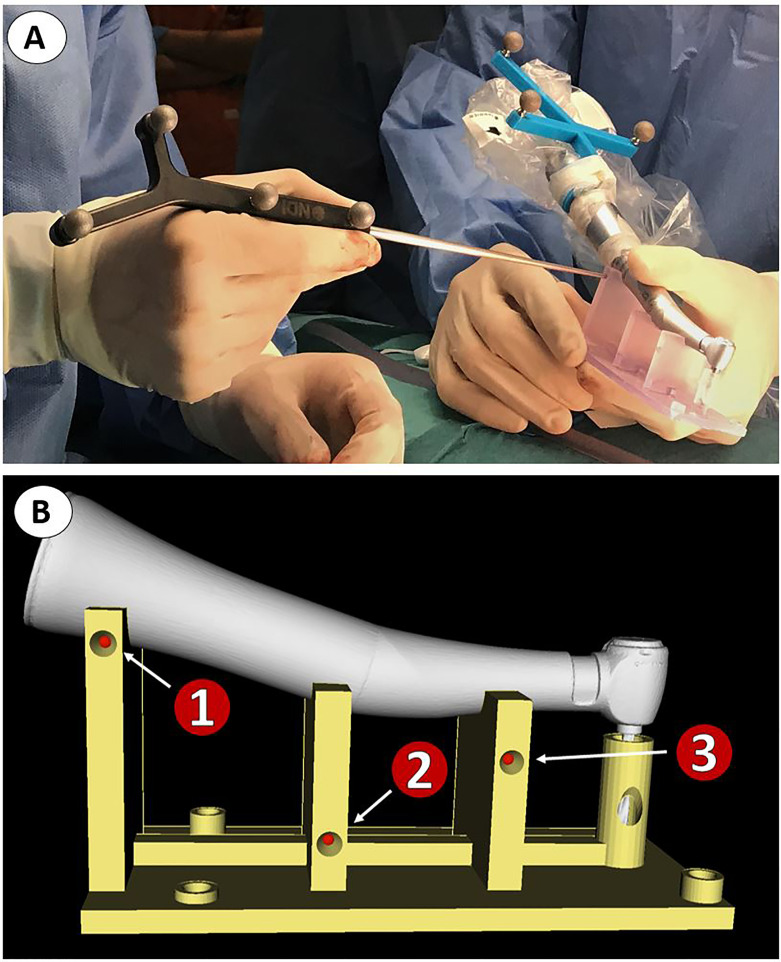
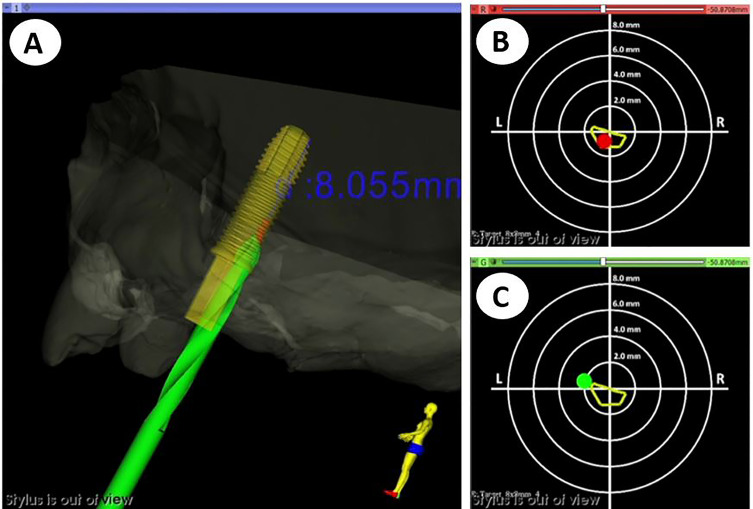
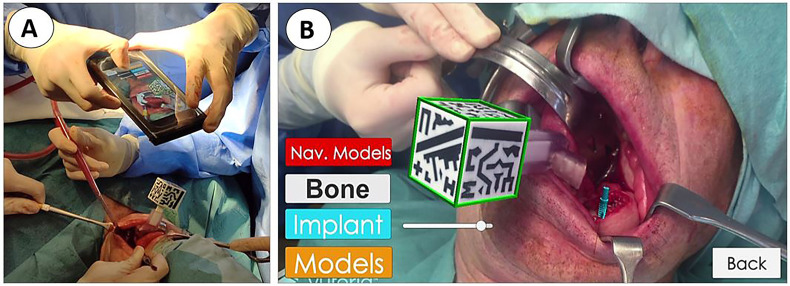
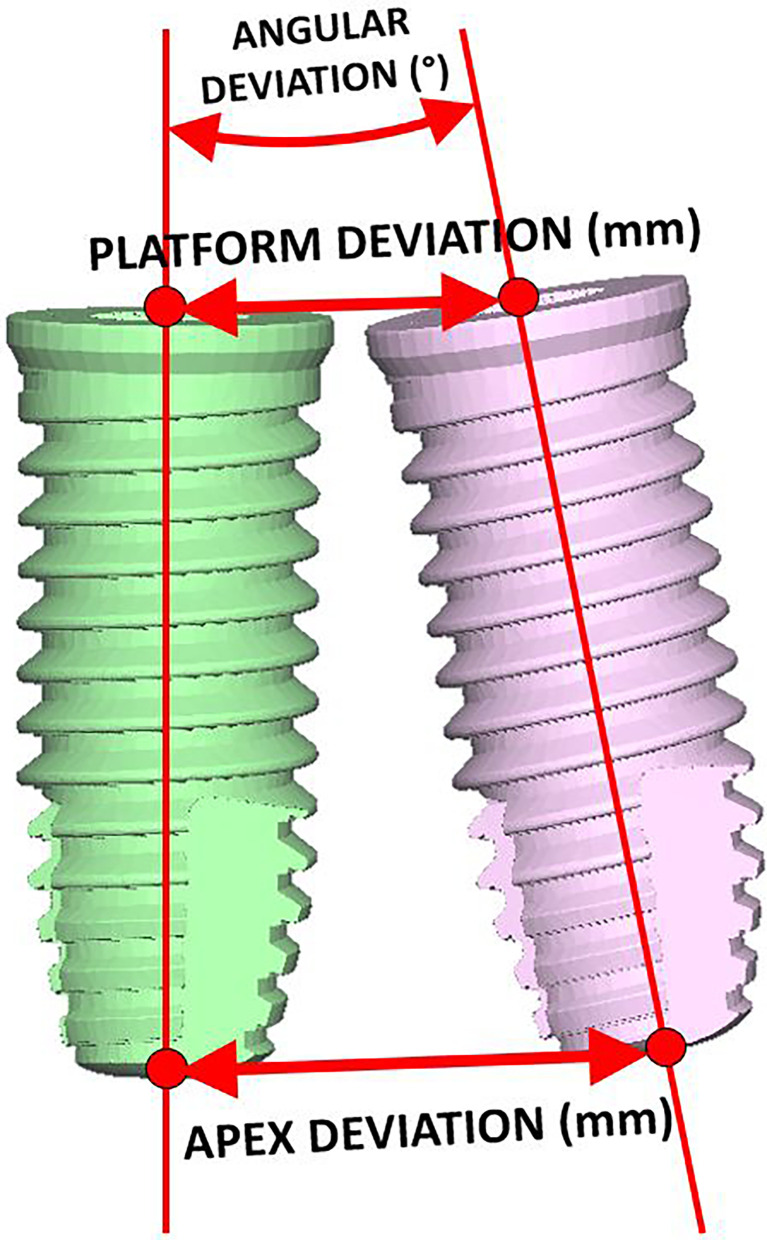
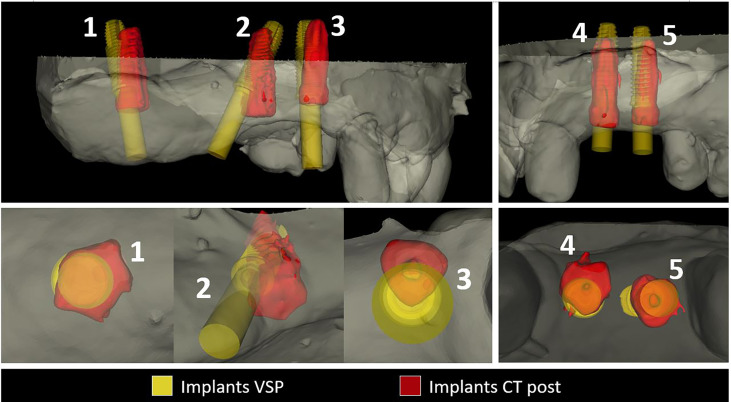
Image-guided surgery, prosthetic-based virtual planning, 3D printing, and CAD/CAM technology are changing head and neck ablative and reconstructive surgical oncology. Due to quality-of-life improvement, dental implant rehabilitation could be considered in every patient treated with curative intent. Accurate implant placement is mandatory for prosthesis long-term stability and success in oncologic patients. We present a prospective study, with a novel workflow, comprising 11 patients reconstructed with free flaps and 56 osseointegrated implants placed in bone flaps or remnant jaws (iliac crest, fibula, radial forearm, anterolateral thigh). Starting from CT data and jaw plaster model scanning, virtual dental prosthesis was designed. Then prosthetically driven dental implacement was also virtually planned and transferred to the patient by means of intraoperative infrared optical navigation (first four patients), and a combination of conventional static teeth supported 3D-printed acrylic guide stent, intraoperative dynamic navigation, and augmented reality for final intraoperative verification (last 7 patients). Coronal, apical, and angular deviation between virtual surgical planning and final guided intraoperative position was measured on each implant. There is a clear learning curve for surgeons when applying guided methods. Initial only-navigated cases achieved low accuracy but were comparable to non-guided freehand positioning due to jig registration instability. Subsequent dynamic navigation cases combining highly stable acrylic static guides as reference and registration markers result in the highest accuracy with a 1-1.5-mm deviation at the insertion point. Smartphone-based augmented reality visualization is a valuable tool for intraoperative visualization and final verification, although it is still a difficult technique for guiding surgery. A fixed screw-retained ideal dental prosthesis was achieved in every case as virtually planned. Implant placement, the final step in free flap oncological reconstruction, could be accurately planned and placed with image-guided surgery, 3D printing, and CAD/CAM technology. The learning curve could be overcome with preclinical laboratory training, but virtually designed and 3D-printed tracer registration stability is crucial for accurate and predictable results. Applying these concepts to our difficult oncologic patient subgroup with deep anatomic alterations ended in comparable results as those reported in non-oncologic patients.
Keywords: 3D printing; augmented reality; computer-aided surgery; dental implants; dynamic navigation; free flaps; static navigation; virtual surgical planning.
Copyright © 2022 Ochandiano, García-Mato, Gonzalez-Alvarez, Moreta-Martinez, Tousidonis, Navarro-Cuellar, Navarro-Cuellar, Salmerón and Pascau.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Mandibular Reconstruction With Fibula Flap and Dental Implants Through Virtual Surgical Planning and Three Different Techniques: Double-Barrel Flap, Implant Dynamic Navigation and CAD/CAM Mesh With Iliac Crest Graft.Front Oncol. 2021 Oct 5;11:719712. doi: 10.3389/fonc.2021.719712. eCollection 2021. Front Oncol. 2021. PMID: 34676161 Free PMC article.
-
Accuracy of dental implant placement using augmented reality-based navigation, static computer assisted implant surgery, and the free-hand method: An in vitro study.J Dent. 2022 Apr;119:104070. doi: 10.1016/j.jdent.2022.104070. Epub 2022 Feb 18. J Dent. 2022. PMID: 35183695
-
A novel mixed reality-guided dental implant placement navigation system based on virtual-actual registration.Comput Biol Med. 2023 Nov;166:107560. doi: 10.1016/j.compbiomed.2023.107560. Epub 2023 Oct 11. Comput Biol Med. 2023. PMID: 37847946
-
The role of computer aided design/computer assisted manufacturing (CAD/CAM) and 3- dimensional printing in head and neck oncologic surgery: A review and future directions.Oral Oncol. 2022 Sep;132:105976. doi: 10.1016/j.oraloncology.2022.105976. Epub 2022 Jul 6. Oral Oncol. 2022. PMID: 35809506 Review.
-
Current state of the art of computer-guided implant surgery.Periodontol 2000. 2017 Feb;73(1):121-133. doi: 10.1111/prd.12175. Periodontol 2000. 2017. PMID: 28000275 Review.
Cited by
-
Comparison of the accuracy of dental implant placement using dynamic and augmented reality-based dynamic navigation: An in vitro study.J Dent Sci. 2024 Jan;19(1):196-202. doi: 10.1016/j.jds.2023.05.006. Epub 2023 May 16. J Dent Sci. 2024. PMID: 38303816 Free PMC article.
-
From Virtual Reality to Reality: Fine-Tuning the Taxonomy for Extended Reality Simulation in Dental Education.Eur J Dent Educ. 2025 Aug;29(3):486-496. doi: 10.1111/eje.13064. Epub 2024 Dec 19. Eur J Dent Educ. 2025. PMID: 39698875 Free PMC article.
-
Comparison of custom-designed oral stents in radiotherapy for head and neck malignancies.Front Bioeng Biotechnol. 2025 Jun 13;13:1544105. doi: 10.3389/fbioe.2025.1544105. eCollection 2025. Front Bioeng Biotechnol. 2025. PMID: 40585848 Free PMC article.
-
Current Trends in the Reconstruction and Rehabilitation of Jaw following Ablative Surgery.Cancers (Basel). 2022 Jul 7;14(14):3308. doi: 10.3390/cancers14143308. Cancers (Basel). 2022. PMID: 35884369 Free PMC article. Review.
-
Accuracy of Augmented Reality-Assisted Navigation in Dental Implant Surgery: Systematic Review and Meta-analysis.J Med Internet Res. 2023 Jan 4;25:e42040. doi: 10.2196/42040. J Med Internet Res. 2023. PMID: 36598798 Free PMC article.
References
-
- Schoen PJ, Raghoebar GM, Bouma J, Reintsema H, Burlage FR, Roodenburg JLN, et al. . Prosthodontic Rehabilitation of Oral Function in Head–Neck Cancer Patients With Dental Implants Placed Simultaneously During Ablative Tumour Surgery: An Assessment of Treatment Outcomes and Quality of Life. Int J Oral Maxillofac Surg (2008) 37(1):8–16. doi: 10.1016/j.ijom.2007.07.015 - DOI - PubMed
-
- Roumanas ED, Garrett N, Blackwell KE, Freymiller E, Abemayor E, Wong WK, et al. . Masticatory and Swallowing Threshold Performances With Conventional and Implant-Supported Prostheses After Mandibular Fibula Free-Flap Reconstruction. J Prosthet Dent (2006) 96(4):289–97. doi: 10.1016/j.prosdent.2006.08.015 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous