

Improved Diagnostic Accuracy of Ameloblastoma and Odontogenic Keratocyst on Cone-Beam CT by Artificial Intelligence
- PMID: 35155194
- PMCID: PMC8828501
- DOI: 10.3389/fonc.2021.793417
Improved Diagnostic Accuracy of Ameloblastoma and Odontogenic Keratocyst on Cone-Beam CT by Artificial Intelligence
Abstract
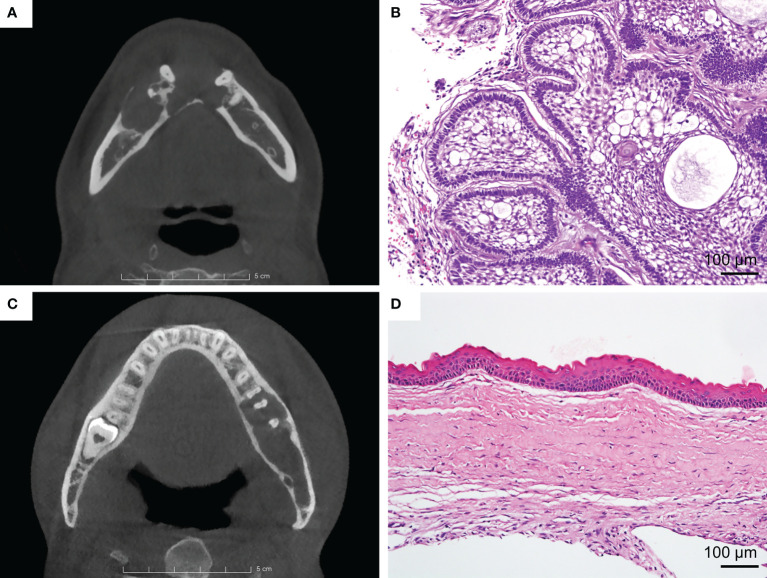
Objective: The purpose of this study was to utilize a convolutional neural network (CNN) to make preoperative differential diagnoses between ameloblastoma (AME) and odontogenic keratocyst (OKC) on cone-beam CT (CBCT).
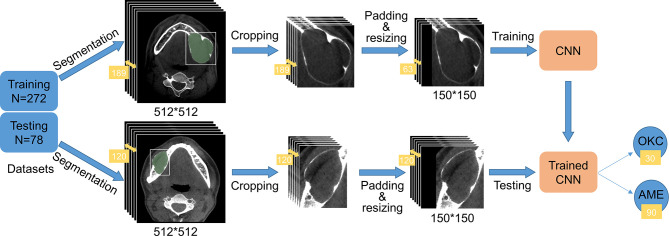
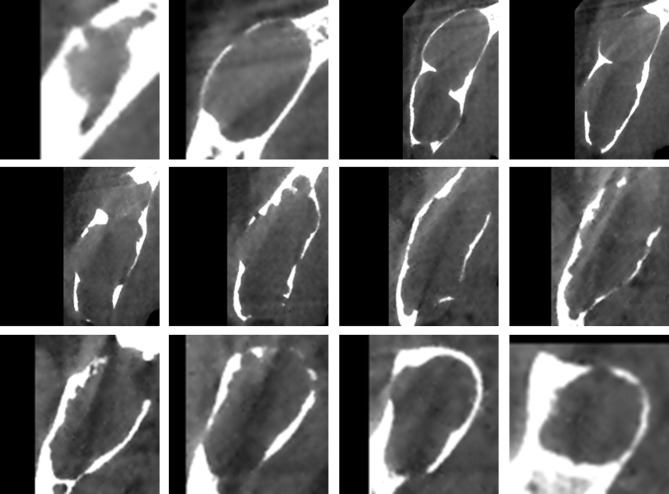
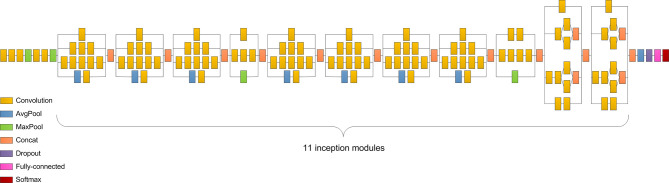
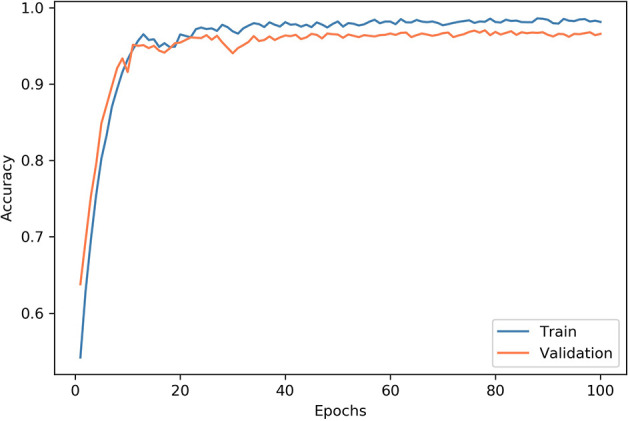
Methods: The CBCT images of 178 AMEs and 172 OKCs were retrospectively retrieved from the Hospital of Stomatology, Wuhan University. The datasets were randomly split into a training dataset of 272 cases and a testing dataset of 78 cases. Slices comprising lesions were retained and then cropped to suitable patches for training. The Inception v3 deep learning algorithm was utilized, and its diagnostic performance was compared with that of oral and maxillofacial surgeons.
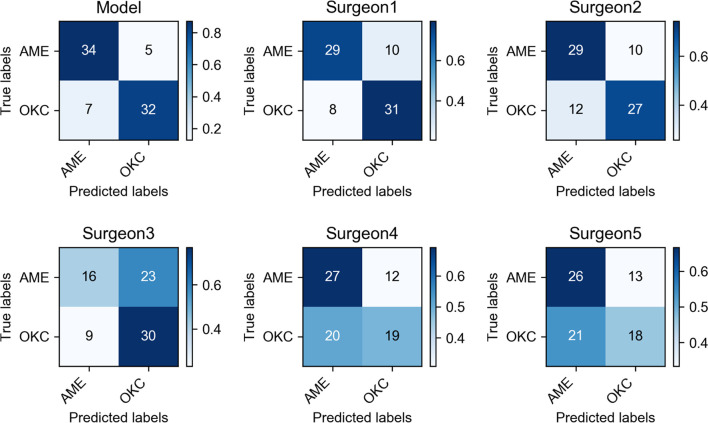
Results: The sensitivity, specificity, accuracy, and F1 score were 87.2%, 82.1%, 84.6%, and 85.0%, respectively. Furthermore, the average scores of the same indexes for 7 senior oral and maxillofacial surgeons were 60.0%, 71.4%, 65.7%, and 63.6%, respectively, and those of 30 junior oral and maxillofacial surgeons were 63.9%, 53.2%, 58.5%, and 60.7%, respectively.
Conclusion: The deep learning model was able to differentiate these two lesions with better diagnostic accuracy than clinical surgeons. The results indicate that the CNN may provide assistance for clinical diagnosis, especially for inexperienced surgeons.
Keywords: Inception v3; ameloblastoma; cone-beam CT; convolutional neural network; deep learning; odontogenic keratocyst.
Copyright © 2022 Chai, Mao, Chen, Sun, Shen, Liu and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Application of Deep Learning in Differential Diagnosis of Ameloblastoma and Odontogenic Keratocyst Based on Panoramic Radiographs].Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2023 Apr;45(2):273-279. doi: 10.3881/j.issn.1000-503X.15139. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2023. PMID: 37157075 Chinese.
-
Application of machine learning in the preoperative radiomic diagnosis of ameloblastoma and odontogenic keratocyst based on cone-beam CT.Dentomaxillofac Radiol. 2024 Jun 28;53(5):316-324. doi: 10.1093/dmfr/twae016. Dentomaxillofac Radiol. 2024. PMID: 38627247 Free PMC article.
-
Differential diagnosis of ameloblastoma and odontogenic keratocyst by machine learning of panoramic radiographs.Int J Comput Assist Radiol Surg. 2021 Mar;16(3):415-422. doi: 10.1007/s11548-021-02309-0. Epub 2021 Feb 6. Int J Comput Assist Radiol Surg. 2021. PMID: 33547985 Free PMC article.
-
Diagnostic capability of artificial intelligence tools for detecting and classifying odontogenic cysts and tumors: a systematic review and meta-analysis.Oral Surg Oral Med Oral Pathol Oral Radiol. 2024 Sep;138(3):414-426. doi: 10.1016/j.oooo.2024.03.004. Epub 2024 Mar 19. Oral Surg Oral Med Oral Pathol Oral Radiol. 2024. PMID: 38845306
-
Accuracy of artificial intelligence in the detection and segmentation of oral and maxillofacial structures using cone-beam computed tomography images: a systematic review and meta-analysis.Pol J Radiol. 2023 May 19;88:e256-e263. doi: 10.5114/pjr.2023.127624. eCollection 2023. Pol J Radiol. 2023. PMID: 37346426 Free PMC article. Review.
Cited by
-
Odontogenic Tumors: A Challenge for Clinical Diagnosis and an Opportunity for AI Innovation.J Dent (Shiraz). 2024 Jun 1;25(2):95-96. doi: 10.30476/dentjods.2024.101237.2284. eCollection 2024 Jun. J Dent (Shiraz). 2024. PMID: 38962076 Free PMC article. No abstract available.
-
Odontogenic cystic lesion segmentation on cone-beam CT using an auto-adapting multi-scaled UNet.Front Oncol. 2024 Jun 12;14:1379624. doi: 10.3389/fonc.2024.1379624. eCollection 2024. Front Oncol. 2024. PMID: 38933446 Free PMC article.
-
Mapping the Use of Artificial Intelligence-Based Image Analysis for Clinical Decision-Making in Dentistry: A Scoping Review.Clin Exp Dent Res. 2024 Dec;10(6):e70035. doi: 10.1002/cre2.70035. Clin Exp Dent Res. 2024. PMID: 39600121 Free PMC article.
-
The Use of Artificial Intelligence in Endodontics.J Dent Res. 2024 Aug;103(9):853-862. doi: 10.1177/00220345241255593. Epub 2024 May 31. J Dent Res. 2024. PMID: 38822561 Free PMC article. Review.
-
Automatic segmentation of ameloblastoma on ct images using deep learning with limited data.BMC Oral Health. 2024 Jan 9;24(1):55. doi: 10.1186/s12903-023-03587-7. BMC Oral Health. 2024. PMID: 38195496 Free PMC article.
References
LinkOut - more resources
Full Text Sources