

The Prognostic Impact of Serum Uric Acid on Disease Severity and 5-Year Mortality in Patients With Idiopathic Pulmonary Artery Hypertension
- PMID: 35155496
- PMCID: PMC8825367
- DOI: 10.3389/fmed.2022.805415
The Prognostic Impact of Serum Uric Acid on Disease Severity and 5-Year Mortality in Patients With Idiopathic Pulmonary Artery Hypertension
Abstract
Background: Serum uric acid (UA) has long been identified as a prognostic factor of adverse outcomes in pulmonary hypertension. However, there remains a paucity of evidence on patients with idiopathic pulmonary artery hypertension (IPAH) in the era of targeted drug therapy. This study aims to explore the impact of serum UA levels on the disease severity and mortality in patients with IPAH.
Methods: Consecutive patients diagnosed with IPAH were enrolled, from which UA levels at baseline and the first follow-up were collected. Patients were divided into groups of "hyperuricemia," which is defined as serum UA level ≥357 μmol/L in women and ≥420 μmol/L in men, and otherwise "normouricemia." The potential relationship between UA and hemodynamics at right heart catheterization was investigated. Associations between UA and survival were evaluated by Kaplan-Meier analysis and Cox proportional hazard modeling.
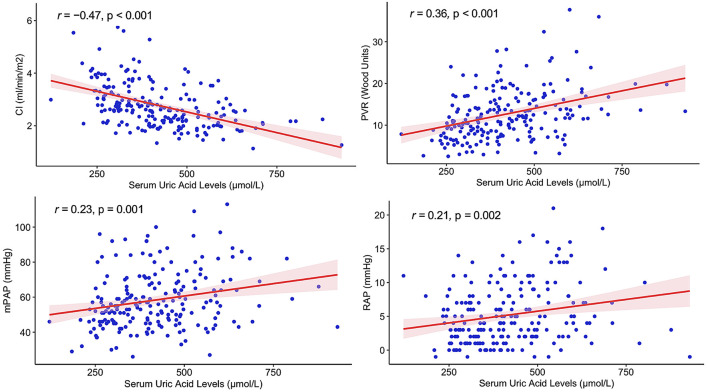
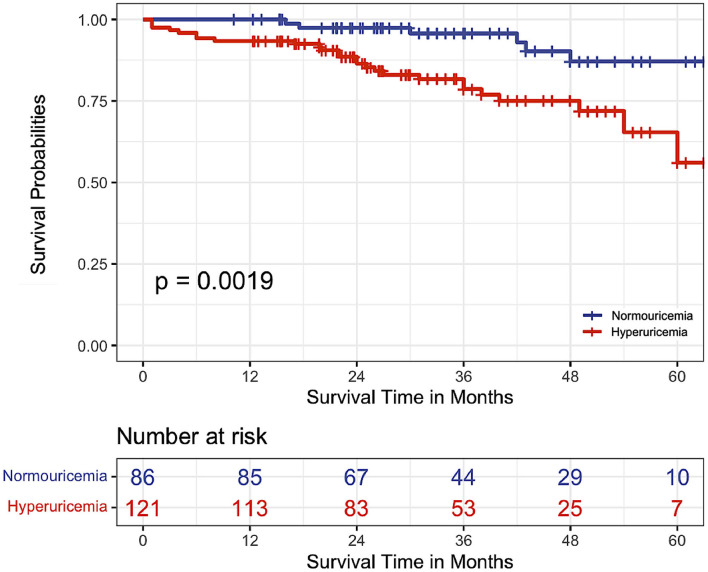
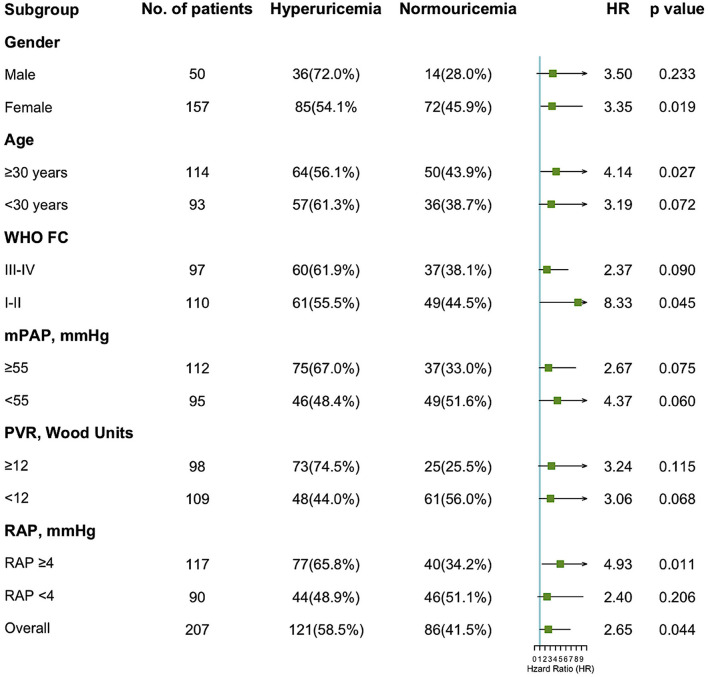
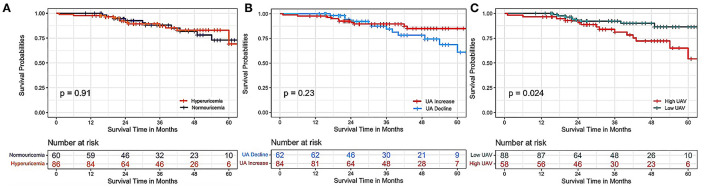
Results: Of 207 patients with IPAH, 121 (58.5%) had hyperuricemia. Higher serum UA levels were associated with lower cardiac index (r = 0.47, p < 0.001) and higher pulmonary vascular resistance (r = 0.36, p < 0.001). During a median follow-up of 34 months, there were 32 deaths recorded, accounting for a 15.5% mortality rate. Patients with hyperuricemia had a significantly lower survival rate than those with normouricemia (log-rank test, p = 0.002). Hyperuricemia at baseline was independently associated with a 2.6-fold increased risk of 5-year death, which was consistent across different subgroups, especially in females and those aged ≥30 years (each p < 0.05). Individuals with higher variability in UA had a higher mortality than those with stable UA (log-rank test, p = 0.024).
Conclusions: Baseline hyperuricemia and high variability in serum UA at first follow-up were related to a higher rate of 5-year mortality in patients with IPAH. Closely detecting the UA levels may aid in the early recognition of IPAH patients at higher mortality risk.
Keywords: IPAH; hyperuricemia; mortality; outcomes; pulmonary hypertension; uric acid.
Copyright © 2022 Yan, Huang, Zhao, Zhao, Tang, Zhang, Li, Duan, Luo and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources