

Comparison between botulinum toxin and steroid septal injection in the treatment of allergic rhinitis
- PMID: 35155778
- PMCID: PMC8823147
- DOI: 10.1002/lio2.726
Comparison between botulinum toxin and steroid septal injection in the treatment of allergic rhinitis
Abstract
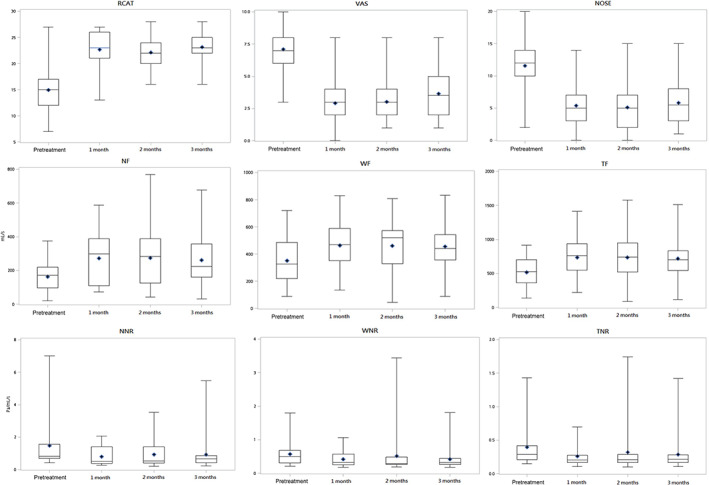
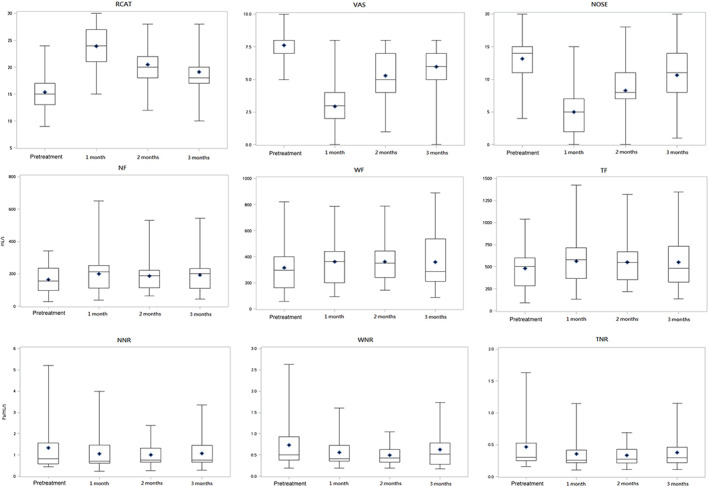
Objective: To compare the effects of botulinum toxin and steroid septal injections in treating allergic rhinitis (AR) by evaluating improvements in the rhinitis control assessment test (RCAT), visual analog scale (VAS), nasal obstruction symptom evaluation (NOSE) scores, and active anterior rhinomanometry (RMM) measurements.
Methods: This prospective, single-blinded cohort study was conducted at the Department of Otolaryngology, Taipei City Hospital between January 2017 and December 2018. Ninety-five patients were randomized to receive botulinum toxin, dexamethasone, or normal saline (group A, group B, and placebo, respectively). The main outcome measures were pretreatment subjective nasal symptoms (RCAT, VAS, and NOSE) and active anterior RMM measurements. All measurements were repeated during posttreatment 1, 2, and 3 months.
Results: No significant difference was observed in pretreatment questionnaire scores and RMM values between the study and placebo groups. The mean posttreatment RCAT, VAS, and NOSE scores after 1 and 2 months significantly improved in the treatment groups compared to placebo. The VAS and NOSE at posttreatment 2 months and RCAT, VAS, and NOSE at posttreatment 3 months were significantly different comparing group A to group B. All RMM parameters showed better values in group A than in group B at 1, 2, and 3 months posttreatment, with significant differences in four parameters in posttreatment 3 months.
Conclusions: Botulinum toxin septal injection is a safe treatment option for AR and improves subjective nasal symptoms for 3 months. Botulinum toxin A injection tended to be more effective than steroid septal injection in terms of duration and degree.Level of Evidence: 2b, individual cohort study.
Keywords: active anterior rhinomanometry; allergic rhinitis; botulinum toxins; septal injection; steroid.
© 2022 The Authors. Laryngoscope Investigative Otolaryngology published by Wiley Periodicals LLC on behalf of The Triological Society.
Conflict of interest statement
The authors declare no potential conflict of interest.
Figures
Similar articles
-
Evaluation of nasal patency by visual analogue scale/nasal obstruction symptom evaluation questionnaires and anterior active rhinomanometry after septoplasty: a retrospective one-year follow-up cohort study.Clin Otolaryngol. 2017 Feb;42(1):53-59. doi: 10.1111/coa.12662. Epub 2016 May 31. Clin Otolaryngol. 2017. PMID: 27102375
-
Septal injection in comparison with inferior turbinates injection of botulinum toxin A in patients with allergic rhinitis.J Res Med Sci. 2013 May;18(5):400-4. J Res Med Sci. 2013. PMID: 24174945 Free PMC article.
-
Assessment of nasal obstruction with rhinomanometry and subjective scales and outcomes of surgical and medical treatment.Acta Otorrinolaringol Esp (Engl Ed). 2017 May-Jun;68(3):145-150. doi: 10.1016/j.otorri.2016.06.007. Epub 2016 Oct 23. Acta Otorrinolaringol Esp (Engl Ed). 2017. PMID: 27780551 English, Spanish.
-
Botolinum toxin in rhinitis: Literature review and posterior nasal injection in allergic rhinitis.Laryngoscope. 2017 Nov;127(11):2447-2454. doi: 10.1002/lary.26616. Epub 2017 Jul 6. Laryngoscope. 2017. PMID: 28681969 Review.
-
Botulinum toxin for chronic rhinitis: A systematic review and meta-analysis.Int Forum Allergy Rhinol. 2021 Nov;11(11):1538-1548. doi: 10.1002/alr.22813. Epub 2021 May 6. Int Forum Allergy Rhinol. 2021. PMID: 33956405
Cited by
-
[Research progress of botulinum toxin type A in the treatment of chronic rhinitis].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2022 Nov;36(11):878-883. doi: 10.13201/j.issn.2096-7993.2022.11.015. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2022. PMID: 36347585 Free PMC article. Review. Chinese.
References
-
- Hwang CY, Chen YJ, Lin MW, et al. Prevalence of atopic dermatitis, allergic rhinitis and asthma in Taiwan: a national study 2000 to 2007. Acta Derm Venereol. 2010;90(6):589‐594. - PubMed
-
- Shaari CM, Sanders I, Wu BL, Biller HF. Rhinorrhea is decreased in dogs after nasal application of botulinum toxin. Otolaryngol Head Neck Surg. 1995;112(4):566‐571. - PubMed
-
- Greiner AN, Meltzer EO. Overview of the treatment of allergic rhinitis and nonallergic rhinopathy. Proc Am Thorac Soc. 2011;8(1):121‐131. - PubMed
-
- Scott AB, Suzuki D. Systemic toxicity of botulinum toxin by intramuscular injection in the monkey. Mov Disord. 1988;3(4):333‐335. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials