

Artificial Intelligent Olfactory System for the Diagnosis of Parkinson's Disease
- PMID: 35155895
- PMCID: PMC8829950
- DOI: 10.1021/acsomega.1c05060
Artificial Intelligent Olfactory System for the Diagnosis of Parkinson's Disease
Abstract
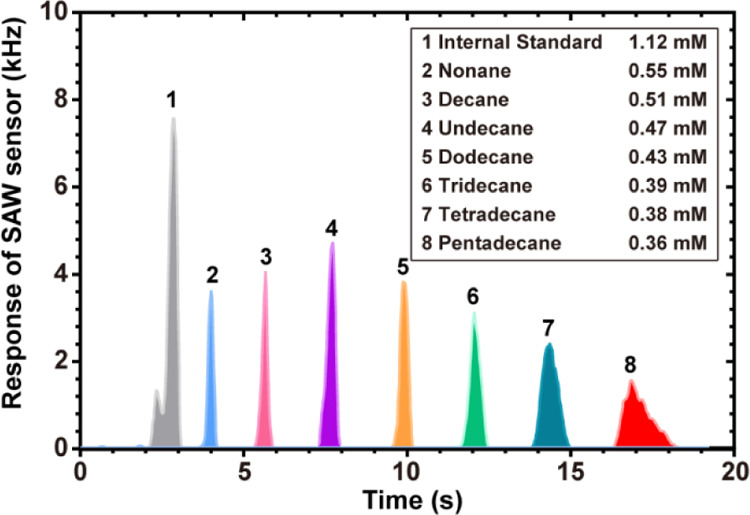
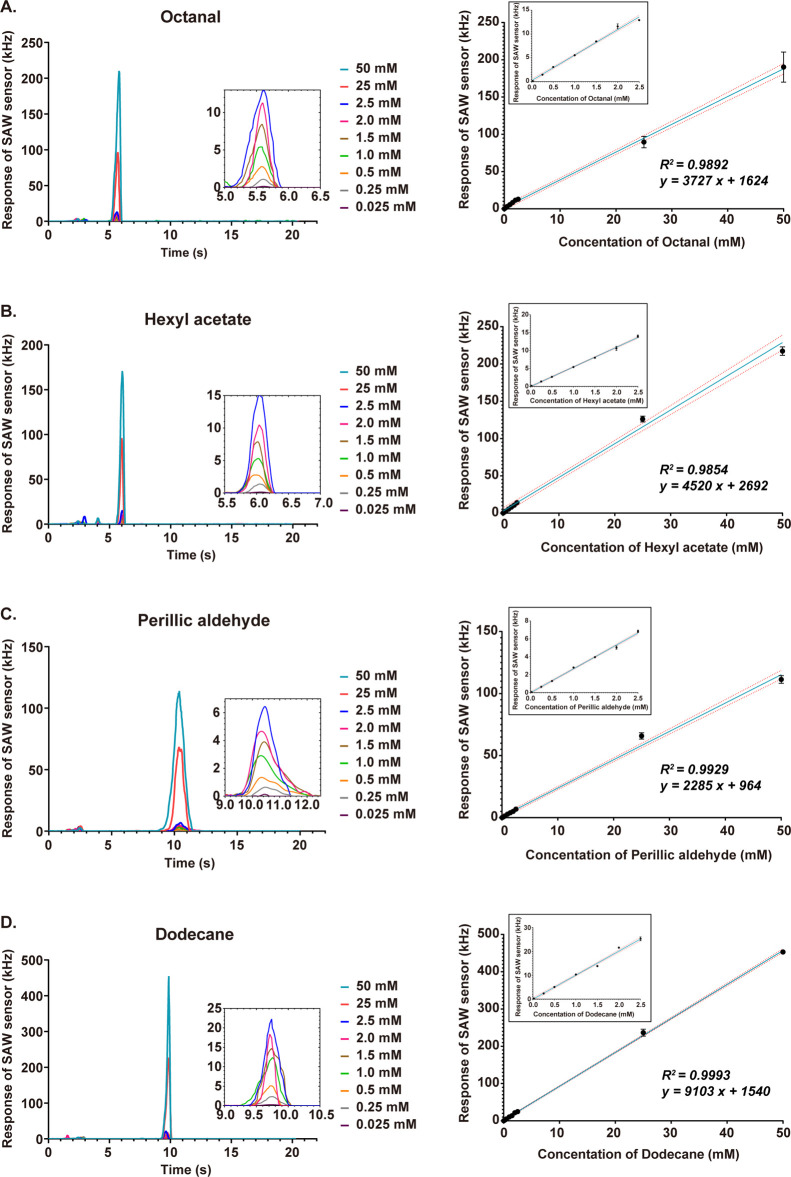
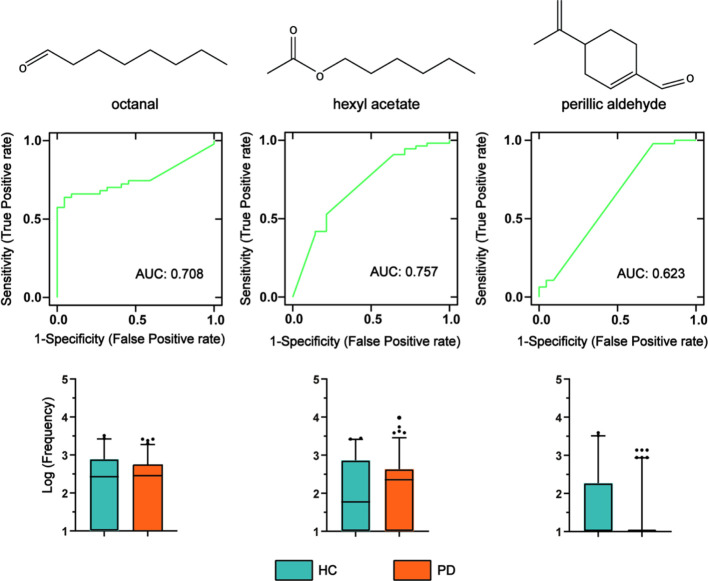
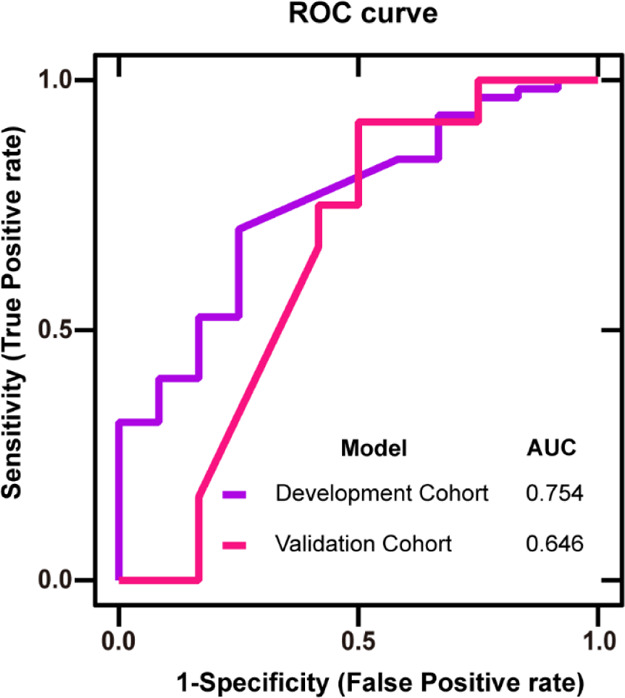
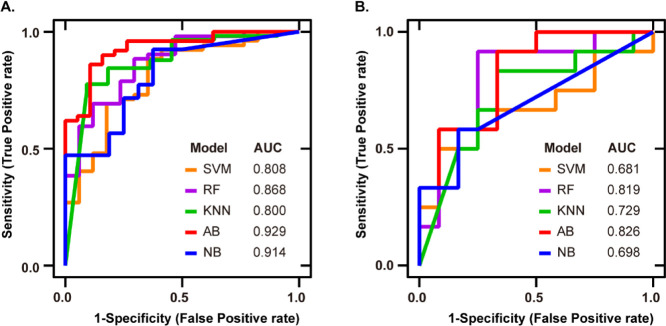
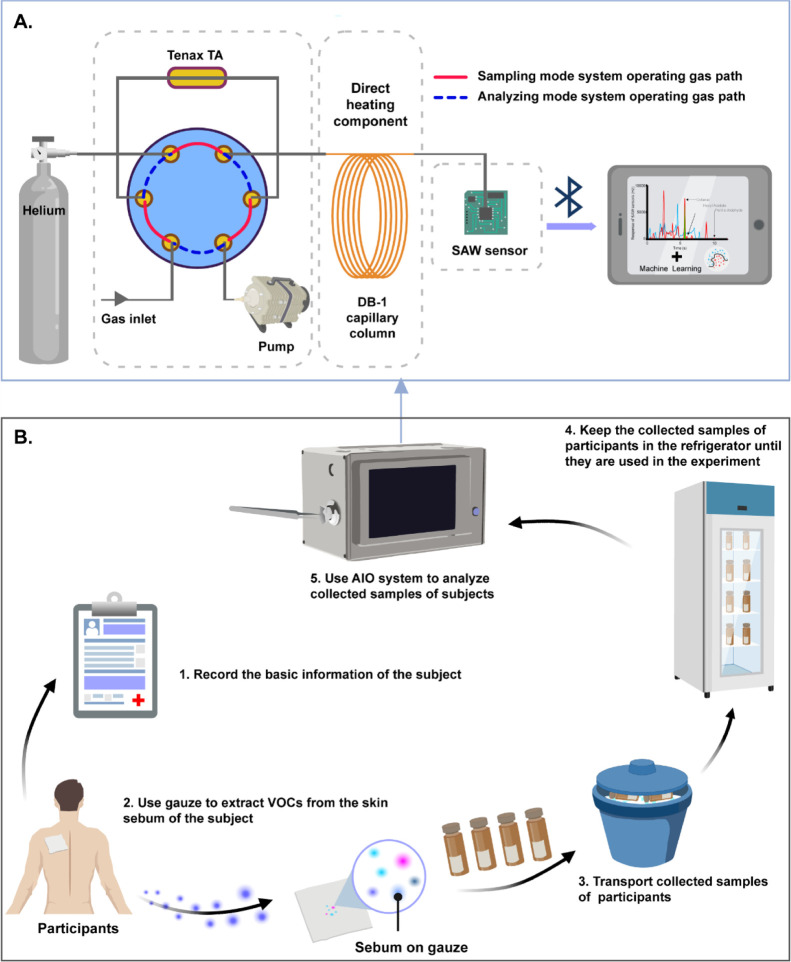
Background: Currently, Parkinson's disease (PD) diagnosis is mainly based on medical history and physical examination, and there is no objective and consistent basis. By the time of diagnosis, the disease would have progressed to the middle and late stages. Pilot studies have shown that a unique smell was present in the skin sebum of PD patients. This increases the possibility of a noninvasive diagnosis of PD using an odor profile. Methods: Fast gas chromatography (GC) combined with a surface acoustic wave sensor with embedded machine learning (ML) algorithms was proposed to establish an artificial intelligent olfactory (AIO) system for the diagnosis of Parkinson's through smell. Sebum samples of 43 PD patients and 44 healthy controls (HCs) from Fourth Affiliated Hospital of Zhejiang University School of Medicine, China, were smelled by the AIO system. Univariate and multivariate methods were used to identify the significant volatile organic compound (VOC) features in the chromatograms. ML algorithms, including support vector machine, random forest (RF), k nearest neighbor (KNN), AdaBoost (AB), and Naive Bayes (NB), were used to distinguish PD patients from HC based on the VOC peaks in the chromatograms of sebum samples. Results: VOC peaks with average retention times of 5.7, 6.0, and 10.6 s, respectively, corresponding to octanal, hexyl acetate, and perillic aldehyde, were significantly different in PD and HC. The accuracy of the classification based on the significant features was 70.8%. Based on the odor profile, the classification had the highest accuracy and F1 of the five models with 0.855 from NB and 0.846 from AB, respectively, in the process of model establishing. The highest specificity and sensitivity of the five classifiers were 91.6% from NB and 91.7% from RF and KNN, respectively, in the evaluating set. Conclusions: The proposed AIO system can be used to diagnose PD through the odor profile of sebum. Using the AIO system is helpful for the screening and diagnosis of PD and is conducive to further tracking and frequent monitoring of the PD treatment process.
© 2022 The Authors. Published by American Chemical Society.
Conflict of interest statement
The authors declare no competing financial interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
