

Influence of Upright Versus Supine Position on Resting and Exercise Hemodynamics in Patients Assessed for Pulmonary Hypertension
- PMID: 35156392
- PMCID: PMC9245795
- DOI: 10.1161/JAHA.121.023839
Influence of Upright Versus Supine Position on Resting and Exercise Hemodynamics in Patients Assessed for Pulmonary Hypertension
Abstract
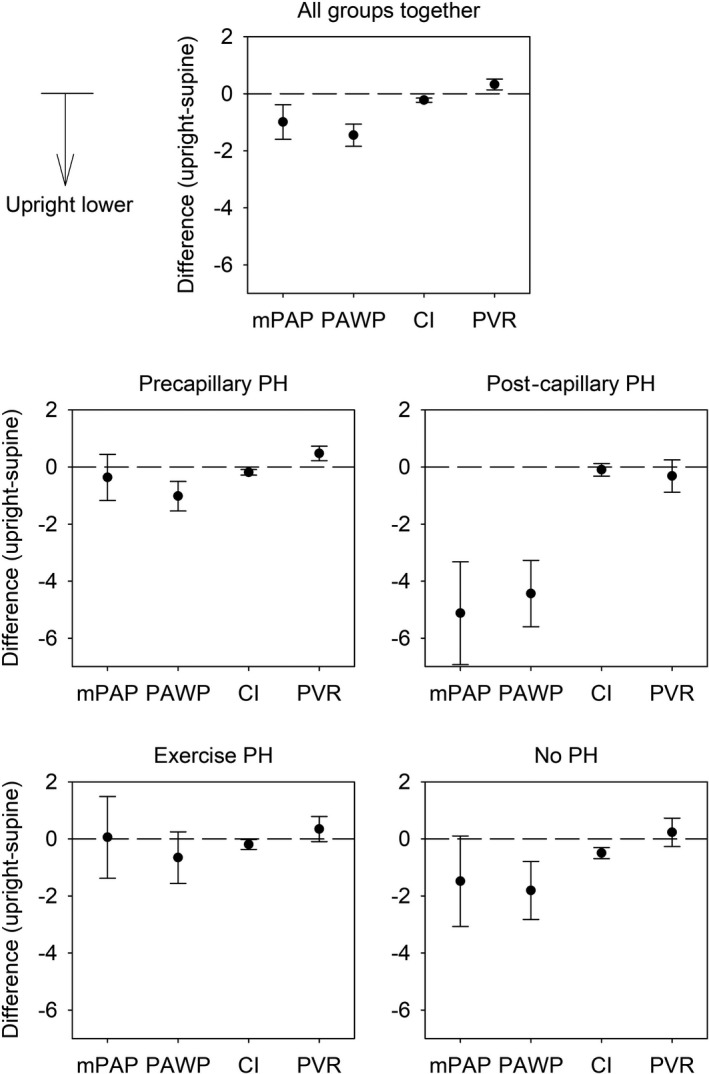
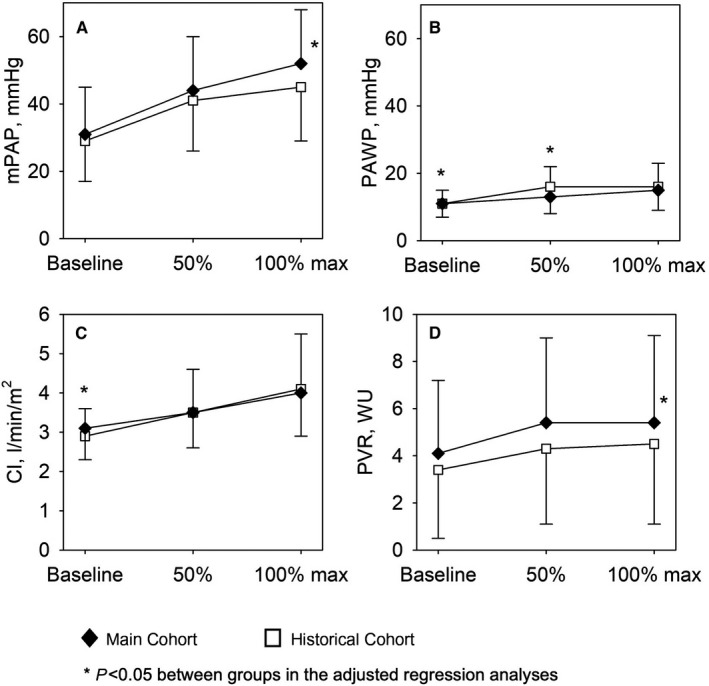
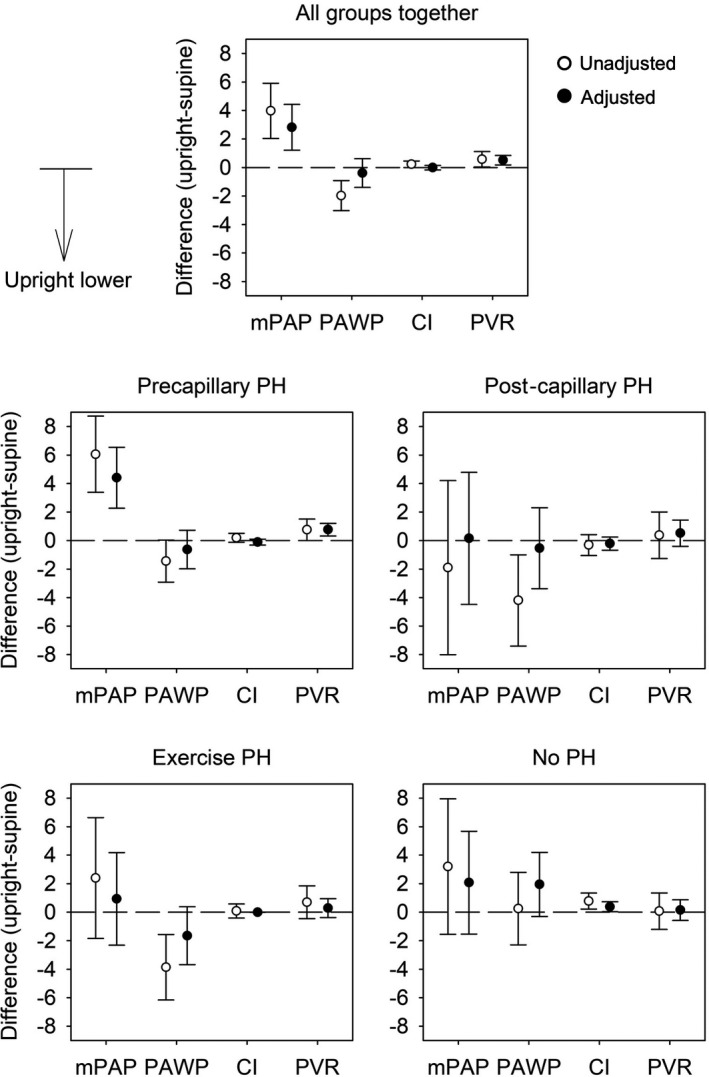
Background The aim of the present work was to study the influence of body position on resting and exercise pulmonary hemodynamics in patients assessed for pulmonary hypertension (PH). Methods and Results Data from 483 patients with suspected PH undergoing right heart catheterization for clinical indications (62% women, age 61±15 years, 246 precapillary PH, 48 postcapillary PH, 106 exercise PH, 83 no PH) were analyzed; 213 patients (main cohort, years 2016-2018) were examined at rest in upright (45°) and supine position, such as under upright exercise. Upright exercise hemodynamics were compared with 270 patients (historical cohort) undergoing supine exercise with the same protocol. Upright versus supine resting data revealed a lower mean pulmonary artery pressure 31±14 versus 32±13 mm Hg, pulmonary artery wedge pressure 11±4 versus 12±5 mm Hg, and cardiac index 2.9±0.7 versus 3.1±0.8 L/min per m2, and higher pulmonary vascular resistance 4.1±3.1 versus 3.9±2.8 Wood P<0.001. Exercise data upright versus supine revealed higher work rates (53±26 versus 33±22 watt), and adjusting for differences in work rate and baseline values, higher end-exercise mean pulmonary artery pressure (52±19 versus 45±16 mm Hg, P=0.001), similar pulmonary artery wedge pressure and cardiac index, higher pulmonary vascular resistance (5.4±3.7 versus 4.5±3.4 Wood units, P=0.002), and higher mean pulmonary artery pressure/cardiac output (7.9±4.7 versus 7.1±4.1 Wood units, P=0.001). Conclusions Body position significantly affects resting and exercise pulmonary hemodynamics with a higher pulmonary vascular resistance of about 10% in upright versus supine position at rest and end-exercise, and should be considered and reported when assessing PH.
Keywords: body position; exercise; hemodynamic; pulmonary hypertension; right heart catheterization.
Figures
References
-
- Galiè N, Humbert M, Vachiery J‐L, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J. 2015;46:903–975. doi: 10.1183/13993003.01032-2015 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
